Downloaded 406 times
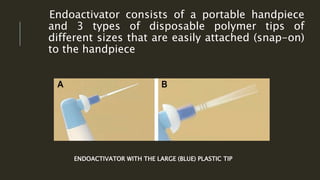
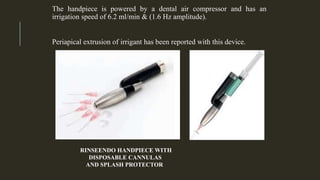
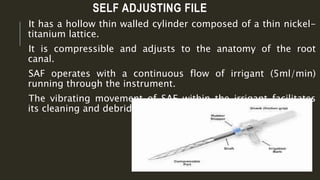

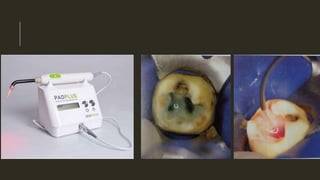


This document discusses various irrigation techniques and devices used in endodontic treatment. It begins by explaining the importance of irrigation to cleanse the complex root canal system. It then describes several manual and machine-assisted irrigation methods including syringe irrigation with needles, brushes, manual dynamic agitation, rotary brushes, sonic and ultrasonic devices, and pressure alternating devices like the EndoVac and RinsEndo systems. The self-adjusting file is also introduced. The document concludes that newer irrigation devices can provide more effective cleaning than conventional needle irrigation.


































































