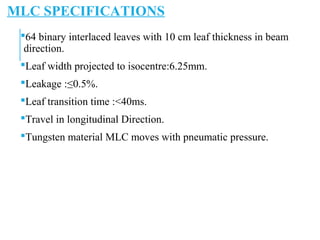
![TOMOTHERAPY CONCEPT
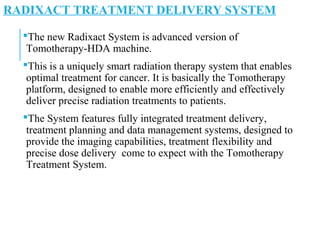
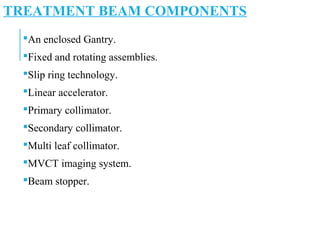
In line short length LA.
Mounted on a continuously rotatable ring directed at its center.
The patient will be slowly translated through the ring.
So Spiral of slit field Radiation, directed at the patient, which
is modulated bi m-MLC 64 binary leaves. Low dose MVCT
images , virtually eliminates the artifacts.
MVCT [3.5MV]detector mounted opposite to the source for
setup registration , treatment planning and verification
purposes.
3D CT image guidance before each treatment.](https://image.slidesharecdn.com/radixact-subrata-190209094021/85/RADIXACT-X9-TOMOTHERAPY-SYSTEM-OVERVIEW-3-320.jpg)
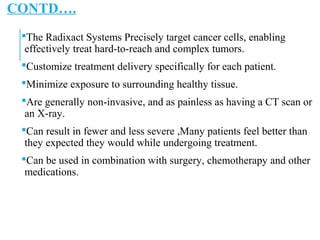
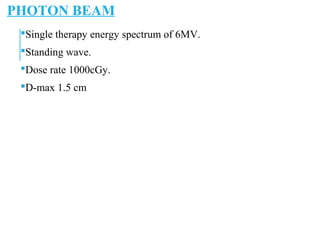
![C-TRUE IMAGING SPECIFICATION
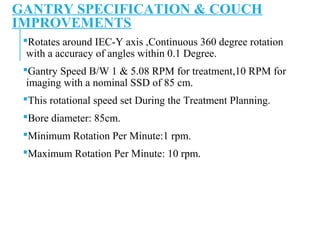
Geometry : Helical Fan Beam.
Image resolution: 512x512(0.76mm Pixels)
Dose/MVCT image : 0.5-3cGy [Depending on resolution and
body thickness & acquisition Pitch]
Detector Configuration : 528 channels ,single row xenon ion
chamber array used for image acquisition.
Field of view: 39 cm diameter.
Source to detector distance: 140 cm.
Image reconstruction with filtered back projection algorithm.
Image reconstruction in Real Time slice by slice at time.](https://image.slidesharecdn.com/radixact-subrata-190209094021/85/RADIXACT-X9-TOMOTHERAPY-SYSTEM-OVERVIEW-13-320.jpg)
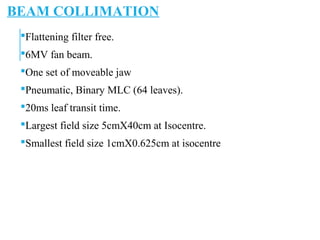

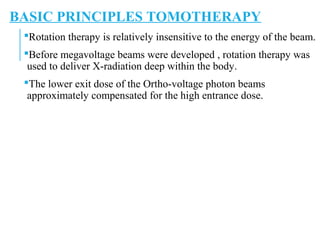
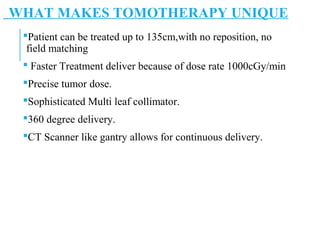
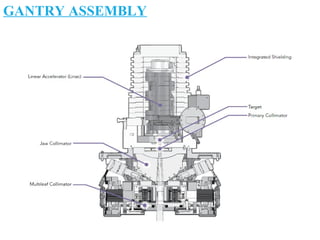
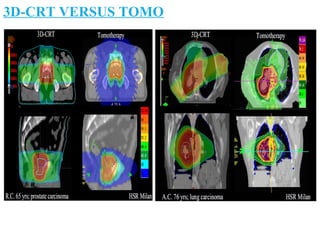
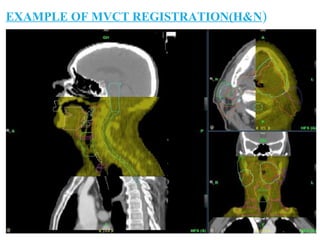
![REGISTRATION
CONSULTATION WITH
RADIATION ONCOLOGIST
PRESCRIPTION OF DOSE
PLAN APPROVAL BY
ONCOLOGIST
PRE VERIFICATION IN
CONSOLE AREA
DOCUMENTATION
TARGET CONTOURING
TREATMENT PLANNING
PREMEDICATION
[IF REQUIRED]
PATIENT SETUPIN
TREATMENT ROOM
CT SIMULATION
COMMENCEMENT OF
TREATMENT
IMMOBILISATION
ACHIEVE CRITERIA FOR
TREATMENT
TREATMENT APPROVAL
SIGN BY ONCOLOGIST &
PHYSICIST
MONITORING THE
PATIENT THROUGHOUT
THE OF TREATMENT
TOMOTHERAPY
WORK FLOW](https://image.slidesharecdn.com/radixact-subrata-190209094021/85/RADIXACT-X9-TOMOTHERAPY-SYSTEM-OVERVIEW-27-320.jpg)


The Radixact X9 Tomotherapy system is an advanced form of radiation therapy utilizing a CT scanner-based platform for delivering precise and flexible treatment to cancer patients. Its unique features include customizable radiation delivery, minimal exposure to healthy tissue, and efficient multi-angle treatment options, making it suitable for complex tumors and various cancers. The system integrates imaging and treatment planning to enable accurate dose delivery and adapt treatment plans as needed.




























![Arc therapy [autosaved] [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/arctherapyautosavedautosaved-150423125828-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)























































