Downloaded 14 times



























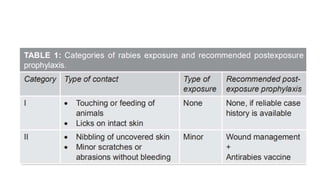
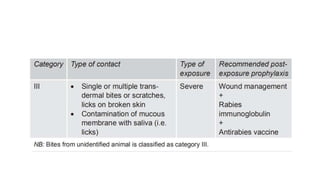










Rabies is a fatal viral infection transmitted through the saliva of infected animals. In children, rabies is commonly transmitted through dog bites, with approximately 35% of India's 20,000 annual rabies deaths occurring in children. Post-exposure prophylaxis, including thorough wound cleansing, vaccine administration, and potentially rabies immunoglobulin, is highly effective if administered promptly after exposure. The standard post-exposure prophylaxis schedule in children consists of 5 doses of rabies vaccine over 28 days.










































































