As natural healthcare practitioners, we all understand the pivotal and complex role that magnesium plays. Required for over 300 biochemical reactions and metabolic functions including cellular signalling, function & energy production, it is no surprise magnesium is one of the most used supplements in a clinician’s toolbox.
Magnesium supplementation is, however, not as straightforward as we are led to believe. With considerations such as carrier, dose and bioavailability to consider, are we really doing clients (and magnesium) justice with a standard ‘go-to’ product?
In this educational webinar, Dr Nina Bailey not only discusses magnesium in clinical practice but, importantly, also uncovers the perils and pitfalls of the magnesium supplement ‘scene’, in the quest to provide clinical excellence, and the important supplemental factors that must be considered to optimise magnesium status and provide clinical efficacy.
Dr Bailey discusses:
1. A brief overview of the clinical implications of magnesium deficiency
2. Magnesium in practice:
-Supporting digestive complaints and overcoming
malabsorption
-The importance of magnesium for structural support
-Supporting energy levels and insulin sensitivity
3. How to ensure clinically effective dosing and supplementation
As natural healthcare practitioners, we all understand the pivotal and complex role that magnesium plays. Required for over 300 biochemical reactions and metabolic functions including cellular signalling, function & energy production, it is no surprise magnesium is one of the most used supplements in a clinician’s toolbox.
Magnesium supplementation is, however, not as straightforward as we are led to believe. With considerations such as carrier, dose and bioavailability to consider, are we really doing clients (and magnesium) justice with a standard ‘go-to’ product?
In this educational webinar, Dr Nina Bailey not only discusses magnesium in clinical practice but, importantly, also uncovers the perils and pitfalls of the magnesium supplement ‘scene’, in the quest to provide clinical excellence, and the important supplemental factors that must be considered to optimise magnesium status and provide clinical efficacy.
Dr Bailey discusses:
1. A brief overview of the clinical implications of magnesium deficiency
2. Magnesium in practice:
-Supporting digestive complaints and overcoming
malabsorption
-The importance of magnesium for structural support
-Supporting energy levels and insulin sensitivity
3. How to ensure clinically effective dosing and supplementation
learning objectives : Pathophysiology of Psoriasis
Common sites with pictures
Pharmacotherapy of Psoriasis
Local Drug therapy
Systemic Drug therapy
Biological therapy
Phototherapy
William F.C. Rigby, MD, discusses rheumatoid arthritis management in this CME activity titled "JAK Inhibitors in Rheumatoid Arthritis: Aligning Pathophysiology, Treatment Advances, and Patient Preference Into a Personalized Approach to Care for Improved Outcomes." For the full presentation, downloadable Practice Aids, monograph, complete CME information, and to apply for credit, please visit us at http://bit.ly/2wcIIc0. CME credit will be available until September 26, 2018.
learning objectives : Pathophysiology of Psoriasis
Common sites with pictures
Pharmacotherapy of Psoriasis
Local Drug therapy
Systemic Drug therapy
Biological therapy
Phototherapy
William F.C. Rigby, MD, discusses rheumatoid arthritis management in this CME activity titled "JAK Inhibitors in Rheumatoid Arthritis: Aligning Pathophysiology, Treatment Advances, and Patient Preference Into a Personalized Approach to Care for Improved Outcomes." For the full presentation, downloadable Practice Aids, monograph, complete CME information, and to apply for credit, please visit us at http://bit.ly/2wcIIc0. CME credit will be available until September 26, 2018.
Biological therapy in rheumatic diseasesSamar Tharwat
Dr.Samar Tharwat ,Lecturer of Internal Medicine (Rheumatology & Immunology)represents a lecture on biological Therapy and its role in various rheumatic diseases.
The drugs included in the presentation are Methotrexate, Cyclosporine, Azathioprine, Cyclophosphamide, Mycophenolate mofetil and Intravenous Immunoglobulin.
It is useful mainly for dermatologists.
Instructions for Submissions thorugh G- Classroom.pptxJheel Barad
This presentation provides a briefing on how to upload submissions and documents in Google Classroom. It was prepared as part of an orientation for new Sainik School in-service teacher trainees. As a training officer, my goal is to ensure that you are comfortable and proficient with this essential tool for managing assignments and fostering student engagement.
2024.06.01 Introducing a competency framework for languag learning materials ...Sandy Millin
http://sandymillin.wordpress.com/iateflwebinar2024
Published classroom materials form the basis of syllabuses, drive teacher professional development, and have a potentially huge influence on learners, teachers and education systems. All teachers also create their own materials, whether a few sentences on a blackboard, a highly-structured fully-realised online course, or anything in between. Despite this, the knowledge and skills needed to create effective language learning materials are rarely part of teacher training, and are mostly learnt by trial and error.
Knowledge and skills frameworks, generally called competency frameworks, for ELT teachers, trainers and managers have existed for a few years now. However, until I created one for my MA dissertation, there wasn’t one drawing together what we need to know and do to be able to effectively produce language learning materials.
This webinar will introduce you to my framework, highlighting the key competencies I identified from my research. It will also show how anybody involved in language teaching (any language, not just English!), teacher training, managing schools or developing language learning materials can benefit from using the framework.
Honest Reviews of Tim Han LMA Course Program.pptxtimhan337
Personal development courses are widely available today, with each one promising life-changing outcomes. Tim Han’s Life Mastery Achievers (LMA) Course has drawn a lot of interest. In addition to offering my frank assessment of Success Insider’s LMA Course, this piece examines the course’s effects via a variety of Tim Han LMA course reviews and Success Insider comments.
Operation “Blue Star” is the only event in the history of Independent India where the state went into war with its own people. Even after about 40 years it is not clear if it was culmination of states anger over people of the region, a political game of power or start of dictatorial chapter in the democratic setup.
The people of Punjab felt alienated from main stream due to denial of their just demands during a long democratic struggle since independence. As it happen all over the word, it led to militant struggle with great loss of lives of military, police and civilian personnel. Killing of Indira Gandhi and massacre of innocent Sikhs in Delhi and other India cities was also associated with this movement.
Synthetic Fiber Construction in lab .pptxPavel ( NSTU)
Synthetic fiber production is a fascinating and complex field that blends chemistry, engineering, and environmental science. By understanding these aspects, students can gain a comprehensive view of synthetic fiber production, its impact on society and the environment, and the potential for future innovations. Synthetic fibers play a crucial role in modern society, impacting various aspects of daily life, industry, and the environment. ynthetic fibers are integral to modern life, offering a range of benefits from cost-effectiveness and versatility to innovative applications and performance characteristics. While they pose environmental challenges, ongoing research and development aim to create more sustainable and eco-friendly alternatives. Understanding the importance of synthetic fibers helps in appreciating their role in the economy, industry, and daily life, while also emphasizing the need for sustainable practices and innovation.
A Strategic Approach: GenAI in EducationPeter Windle
Artificial Intelligence (AI) technologies such as Generative AI, Image Generators and Large Language Models have had a dramatic impact on teaching, learning and assessment over the past 18 months. The most immediate threat AI posed was to Academic Integrity with Higher Education Institutes (HEIs) focusing their efforts on combating the use of GenAI in assessment. Guidelines were developed for staff and students, policies put in place too. Innovative educators have forged paths in the use of Generative AI for teaching, learning and assessments leading to pockets of transformation springing up across HEIs, often with little or no top-down guidance, support or direction.
This Gasta posits a strategic approach to integrating AI into HEIs to prepare staff, students and the curriculum for an evolving world and workplace. We will highlight the advantages of working with these technologies beyond the realm of teaching, learning and assessment by considering prompt engineering skills, industry impact, curriculum changes, and the need for staff upskilling. In contrast, not engaging strategically with Generative AI poses risks, including falling behind peers, missed opportunities and failing to ensure our graduates remain employable. The rapid evolution of AI technologies necessitates a proactive and strategic approach if we are to remain relevant.
BÀI TẬP BỔ TRỢ TIẾNG ANH GLOBAL SUCCESS LỚP 3 - CẢ NĂM (CÓ FILE NGHE VÀ ĐÁP Á...
RHEUMATOID ARTHRITIS (VK)
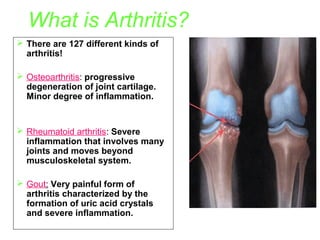
1. What is Arthritis?
There are 127 different kinds of
arthritis!
Osteoarthritis: progressive
degeneration of joint cartilage.
Minor degree of inflammation.
Rheumatoid arthritis: Severe
inflammation that involves many
joints and moves beyond
musculoskeletal system.
Gout: Very painful form of
arthritis characterized by the
formation of uric acid crystals
and severe inflammation.
2. Rheumatoid arthritisChronic progressive, autoimmune disease in
which there is joint inflammation, synovial
proliferation, and destruction (crippling) of
articular cartilages with waxing and waning
course.
INFLAMMATORY MEDIATORS-
Cytokines
Interleukin 1
TNF-alpha
3. Autoimmune
IgM activates complements and release infl. Mediators
Neutrophil infiltration
Release of Lysosomal enzymes
PGs
Damage to cartilage, bone errosion
vasodilatation
edema & pain
4.
5.
6.
7. • Diagnosis
–
–
–
•
Early diagnosis is the first step to easy control
History
Physical examination
Findings
1.Morning stiffness >1hour
2.Symetrical joint swelling for 6 weeks.
3.Swelling in 3 or more joint areas lasting for
6 weeks or more.
4.Rheumatoid nodule.
5.Positve RF.
6.Radiographic erosions.
8. The treatment approach:
1. Aims to reduce & possibly prevent damage to the joints & other
organs.
2. Relief of pain –primary aim.
3. Rx of pathology-
Arrest of disease process
- Modification of disease process
-
Nonpharmacological therapy:
o Traditional physical therapy includes-heat & cold therapy
o Motion exercises, Aerobic exercise with muscle strength.
Pharmacological therapy:
o NSAIDs
o DISEASE MODIFYING ANTIRHEUMATIC DRUGS
[DMARDs]
o Adjuvant: GLUCOCORTICOIDS
9. NSAIDs• Used in first; they afford symptomatic relief of
pain, swelling, morning stiffness, immobility.
• Donot arrest disease process.
Diclofenac sodium (75-100mg BD)
Ibuprofen
(200-400mg TDS)
Naproxen
(500mg single dose)
Aspirin
(3-5g/day)
Indomethacin
Special precautions
- Peptic
ulcer
-Bleeding disorder
10. DISEASE MODIFYING ANTIRHEUMATIC
DRUGS [DMARDs]
• Suppress the rheumatoid process i.e.
arrest the basic process of joint
destruction
• Bring about remission.
• Also called as SAARDs
»Contd.,
11. DMARDs
•
1.Methotrexate (Mtx.)
•
2. Agents used in mild disease or in combination with MTX.
•
•
•
•
3.Traditional DMARDs -(limited used currently)
•
•
•
•
Gold salts (Aurothiomalate sodium)…..X
d-Penicillamine………………………..X
Azathioprine
4. Biological agents
•
•
•
•
Hydroxychloroquine
Sulfasalazine
Minocycline
Cyclosporine
Infliximab
Leflunomide
Methoterxate, Azathioprine, Cyclosporine are IMMUNOSUPPRESANT
Leflunomide IMMUNO MODULATOR
12. METHOTREXATE (Mtx)
• An anti metabolite (inhibit dihydrofolate reductase)
inhibits folic acid synthesis.
• 1st line DMARD at present
• RA-Primary MOA is anti-inflammatory rather than
antimetabolites -Inhibit cytokine production, cell
mediated immune reaction, chemotaxis.
• Dose-7.5-10 mg oral weekly.
• Onset of symptom relief is relatively rapid –
preferred for initial treatment
»Contd.,
13. • PK- Oral BV of Mtx is variable, may effected by food
- Excretions is dec. in renal disease pt.
• S/E-GIT distress (parenteral therapy effective to reduce
30mg/wk. i.v, less expensive.)
-Oral ulcer
-Hair loss
-Pneumonia (dec. By use of FA)
-Dose dependent progressive liver damage
14. Hydroxychloroquine
• Antimalarial
• Antirheumatic-found to induce remission in 50% patients.
• MOA-inhibit inflammatory cells: monocytes interleukins,
B lymphocytes.
• RA- long periods
• Dose-200mg bd
• Combined with MTX.
• S/ERetinal damage
Corneal opacities
Neuropathy, Myopathy
Rash
Graying of hairs
Irritable bowel syndrome
15. Sulfasalazine
• Combination of sulphapyridine and 5 aminosalicylic
acid
• Inhibits generation of superoxides and cytokines by
the inflammatory cells.
• Efficacy is equal to chloroquine.
• 1-3g/day (3divided dose)
• Few adverse effect / good alternative for Mtx
Minocycline
• Group III broad spectrum antibiotic inhibit
arthritic inflammation.
• Used in com. With MTX.
16. Gold salts (Aurothiomalate sodium)
• Introduced in 1929.
• Gold is most effective agent for arresting
rheumatic process and preventing
involvement of additional joints.
• It reduce chemotaxis, phagocytosis,
macrophages and lysosomal activity and
inhibit cell mediated immunity
• Benefit - 4-6wks
• Starting dose10mg im/wk gradually inc. to
50mg/im/wk up to 1g.then maintain
50mg /im/ for few months.
»Contd.,
17. • PK:-Gold is heavily bound to plasma and
tissue proteins, specially in kidney, stay in
the body for years
• Toxicity:– Vasodilatation, postural hypotension
– Dermtitis, pruritic rash,
– Albuminuria
– Hepatitis, peripheral neuritis, pulmonary
fibrosis
– Eosinophilia , bone marrow suppression
18. D-Penicillamine
• Copper chelating agent
• Gold compound like action but less
efficacious.
• Toxicity is similar like gold
• Toxicity: Rash, Proteinurea, Kidney damage,
bone marrow depression
• Dose: Start with 125-250mg OD, then 250mg
BD.
19. Azathioprine
• Purine antimetabolite
• Potent suppressant of cell mediated
immunity
• Affect differentiation and function of T-cells
and natural killer cells
• Remission in RA is less but some cases
not responding to gold may respond to it.
• Given along with corticosteroid
• Dose: 2.5-5mg/kg/day
20. 4.Biological agents
Infliximab• Chimeric IgG1-kappa monoclonal antibody
• Anti TNF antibodies
• Binds to soluble, bound both the forms of TNF
and thus causes dose dependent neutralization
of TNF alpha.
• Useful in patients resistant to DMARDs and
Methotrexate.
• Given IV, half life 8-12 days.
• A/E: N,V,H and coughing.
other use-Crohn’s disease.
»Contd.,
21. Entanercept
• Dimer consisting of TNF receptor joined to Fc
domain of human IgG…..binds to TNFα & β.
• Given by SC route thrice a wk.
• Effective in juvenile RA where Infliximab is found
ineffective.
Levamisole
• Antihelminthic in a dose of 150 mg.
• MOA-unknown
• A/E- Agranulocytosis
22. Leflunomide:
• Recently introduced immunomodulator
• It inhibits proliferation of activated lymphocytes in
patients with active RA.
• Arthritic symptoms are suppressed and radiological
progression is retarded
• It is rapidly converted in the body to active
metabolite, which inhibits dihydroorotate
dehydrogenase and pyrimidine synthesis in actively
growing cells.
»Contd.,
23. • It is alternative for MTX or Sulfasalazine
• Dose: Loading dose of 100mg daily for
3days followed by 20mg OD (t1/2 2 wks)
• S/E: Elevation of liver enzymes, renal
impairment and teratogenic effect
23
24. • Adverse effects:- D, H, N, rashes, loss of
hair, thrombocytopenia, chest infection
• C/I:children, pregnant and lactating
women.
25. Corticosteriods
• Potent immunosuppressants and
antiinflammatory drugs.
• Inducted at any stage in RA.
• They do not arrest the rheumatoid process nor
prevent erosions.
• Long term use of corticosteroid carries serious
disadvantages.. Low dose 5-10mg
• High dose employed over short periods in cases
with severe systemic manifestations.
Editor's Notes
Exercise recommendations are tricky for arthritis. Research is changing quickly on this topic. Mention that fibromyalgia is also increasingly diagnosed (refer to fact sheets).
(RF) is the autoantibody (antibody directed against an organism's own tissues) that is most relevant in rheumatoid arthritis.[1] It is defined as an antibody against the Fc portion of IgG. RF and IgG join to form immune complexes that contribute to the disease process
Raised rheumatoid factor levels of 25-50 IU/mL, 50.1-100 IU/mL and more than 100 IU/mL were compared with normal levels (less than 25 IU/mL).
slow acting anti-rheumatic drugs (SAARDs),,,, A period during which symptoms of disease are reduced (partial remission) or disappear (complete remission). With regard to cancer, remission means there is no sign of it on scans or when the doctor examines you. Doctors use the word 'remission' instead of cure when talking about cancer because they cannot be sure that there are no cancer cells at all in the body. So the cancer could come back in the future, although there is no sign of it at the time.
Chemotaxis is the phenomenon whereby somatic cells, bacteria, and other single-cell or multicellular organisms direct their movements according to certain chemicals in their environment. This is important for bacteria to find food (for example, glucose) by swimming towards the highest concentration of food molecules, or to flee from poisons (for example, phenol). In multicellular organisms, chemotaxis is critical to early development (e.g. movement of sperm towards the egg during fertilization) and subsequent phases of development (e.g. migration of neurons orlymphocytes) as well as in normal function. In addition, it has been recognized that mechanisms that allow chemotaxis in animals can be subverted during cancer metastasis.