Rheumatoid arthritis and gout.ppt
•Download as PPT, PDF•
0 likes•16 views

Rheumatoid arthritis and gout

Recommended
Recommended
More Related Content
Similar to Rheumatoid arthritis and gout.ppt
Similar to Rheumatoid arthritis and gout.ppt (20)
Recently uploaded
Recently uploaded (20)
Rheumatoid arthritis and gout.ppt
- 1. 1
- 2. 2
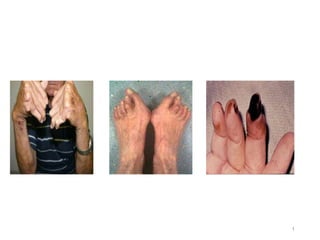
- 3. Rheumatoid arthritis (RA) • Chronic systemic inflammatory disorder that may affect many tissue and organs – Skin, Blood vessels, Heart, Lungs and muscles but principally attack the JOINTS, producing a non suppurative proliferative synovitis that often progresses to the destruction of the articular cartilage and ankylosis of the joints 3
- 4. Rheumatoid arthritis (RA) • Autoimmune disorder • Unknown etiology • Genetics • Environmental • Possible infectious component Autoimmune disease • Joint inflammation • Synovial proliferation • Destruction of articular cartilage • Inflammatory mediators induce immune system in RA; • TNFα, Interleukin 1, Nitric oxide, prostaglandins (PGE2, LTB4) metalloproteinase 4
- 5. 5
- 6. 6
- 7. Classification Disease modifying antirheumatic drugs (DMARDs) A. Nonbiological drugs 1. Immunosuppressants: Methotrexate, Azathioprine, Cyclosporine 2. Sulfasalazine 3. Chloroquine or Hydroxychloroquine 4. Leflunomide B. Biological agents 1. TNFα inhibitors: Etanercept, Infliximab, Adalimumab 2. IL-1 antagonist: Anakinra II. Adjuvant drugs Corticosteroids: Prednisolone and others (Gold and penicillamine are obsolete DMARDs.) 7
- 8. Classification of anti-rheumatic drugs A. Anti-inflammatory drugs • Aspirin and others COX 2 Specific drugs B. Anti-inflammatory drug without Analgesic activity • (Adjuvant drugs) Corticosteroids; Prednisolone 8
- 9. Classification of anti-rheumatic drugs Contd.. C. Disease Modifying Anti-rheumatic Drugs (DMARD) • Immunosuppressants: Methotrexate, Azathioprine, Cyclosporine, Tacrolimus, Cyclophosphamide, Chlorambucil • Sulfasalazine • Chloroquine or Hydroxychloroquine • Leflunomide • Gold Sod, Thiomalate, Auranofin • d-Penicillamine 9
- 10. D. TNFα Blocker • Infliximab, Etanercept, Adalimumab E. Interleukin-1 receptor Antagonist • Anakinra 10
- 11. 1. Gold • Reduces Chemotaxis, Phagocytosis, Macrophage and lysosomal activity, Monocyte differentiation, Inhibits cell mediated immunity (CMI), Rheumatoid factor levels, ESR are lowered • Exact mechanism of action is not known • Indicated in rapidly progressing forms of rheumatoid arthritis along NSAIDs • Effective in psoriatic arthropathy Gold sod. thiomalate (Aurothiomalate sod., contains 50% gold and is water soluble) • Starting dose 10 mg i.m./week is gradually increased to 50 mg i.m/week; till remission occurs or a maximum total dose 1 g • Then maintain with 50 mg i.m./month for few months or as long as tolerated • Heavily bound to plasma and tissue proteins, especially in kidney: stays in the body for years 11
- 12. Toxicity of Gold • Vasodilatation and postural hypotension occurs acutely • Dermatitis, pruritic rash, stomatitis; most common, rarely exfoliative dermatitis • Albuminuria secondary to membranous glomerulo-nephritis; in 10% patients • Hepatitis, peripheral neuritis, encephalopathy and pulmonary fibrosis; less common • Eosinophilia common; bone marrow suppression infrequent but serious Contraindication • Kidney, liver and skin disease • Colitis • Pregnancy • Lactation • In combination with other potentially bone marrow toxic drugs 12
- 13. d-PeniciIlamine • A copper chelating agent with gold like action in RA, but less efficacious; bony erosions do not heal • Does not offer any advantage in terms of toxicity; not favoured now • Penicillamine increases soluble collagen and is the preferred drug for stage II and III scleroderma • Toxicity is similar to gold • Rash, proteinuria, kidney damage, bone marrow depression Anorexia, nausea and loss of taste sensation • Patients develop antinuclear antibodies; SLE or myasthenia gravis may be precipitated • Dose: start with 250 mg OD, then 250 mg BD • ARTAMIN® 150, 250 mg cap 13
- 14. Chloroquine and hydroxychloroquine • Anti-malarial drugs • Remission in 50% patients of RA • Less effective than gold, often used first in milder non-erosive disease because of less ADRs profile • Mechanism of action is not known • Found to reduce Monocyte Interleukin I, Inhibiting B-lymphocytes, May interfered with antigen processing • Long Term use in RA • Retinal damage • Corneal opacity • less common & reversible in hydroxyl-chloroquine • Preferred to Chloroquine • Rashes, graying of hair, irritable bowel syndrome, myopathy & neuropathy • Dose: Hydroxychloroquine 400 mg/day for 4-6 weeks, followed by 200-400 mg/day for maintenance 14
- 15. Sulfasalazine • Sulfapyridine + 5-amino salicylic acid (5-ASA) • Anti-inflammatory; primarily used in ulcerative colitis • Suppress the RA • Efficacy appears to be similar to hydroxy-chloroquine, • Better tolerated than gold or Penicillamine • 1-3 g/day in 2-3 portions The mechanism of action is not known • Sulfapyridine split off in the colon absorbed, systemically appears to be the active moiety (contrast ulcerative colitis in which 5-ASA acting locally in the colon is the active component) • Generation of superoxide radicals and cytokine elaboration by inflammatory cells may be suppress 15
- 16. Methotrexate (Mtx) • Inflammatory property • Beneficial effects in RA are probably related to inhibition of cytokine production, • Chemotaxis and cell mediated immune reaction • Induction of oral low dose (2.5-15mg) weekly Mtx regimen improved acceptability of this drug in RA • At low dose methotrexate is not immuno suppressant • Onset of symptom relief is more rapid than with other DMARD preferred for initial treatment, frequently used now • Remission and healing of erosions achieved in lesser percentage of cases than with gold 16
- 17. Methotrexate (Mtx) Contd….. • Oral bioavailability of Mtx is variable and may be affected by food • Excretion hindered in renal disease: not recommended for such patients • Nodulosis; major side effect of low dose Mtx regimen • Prolonged therapy dose dependent progressive liver damage leading to cirrhosis occurs in - 1/3 patients (this is not seen with short courses used in cancer) • Incidence of chest infection is increased 17
- 18. Cyclosporine • T-cell specific immunosuppressant; effective in RA • Cyclic peptide with 11 amino acids • ↓ Clonal proliferation of T cells • ↓ induction of clonal proliferation of cytotoxic T cells • ↓ Cell mediated immunity by ↓ function of effector T cells • ↓ T cell dependent B cell responses 18
- 19. • Can be given orally or by iv, • t1/2 is 24hrs • Accumulates in the tissues • May be employed in refractory cases of RA • Dose: 2.5-5 mg/kg/day Adverse Drug effects • Renal toxicity which is accentuated by NSAIDs precludes its routine use • Hepatotoxicity & hypertension • Anorexia, lethargy, hirsutism, tremor, parasthesia, gum hepertrophy, GI disturbances • No bone marrow depression 19
- 20. Corticosteroids • Potent immunosuppressant and anti-inflammatory • Can be used at any stage in rheumatoid arthritis along with first or second line drugs • Do not arrest the rheumatoid process nor prevent erosions 20
- 21. Corticosteroids Contd…. • Their long term use carries serious disadvantages • Therefore, either low doses (5-10 mg prednisolone or equivalent) are used to supplement NSAIDs • Once used in this manner, it is difficult to withdraw steroids - exacerbation is precipitated • High doses are employed over short periods in cases with severe systemic manifestations (organ threatening disease, vasculitis) 21
- 22. TNFα antagonists in RA Infliximab • Protein, Chimeric monoclonal anti TNFα antibody • Binds to soluble and membrane bound TNFα • Given i.v once in 4 - 8 weeks • t1/2 = 8-12 days • Also effective in Crohn’s disease ADRs; • Fever, Chills, urticaria, Skin rashes, bronchospasm, & rarely anaphylaxis on i.v infusion • Worsening CHF & respiratory infections 22
- 23. Etanercept •Protein Dimer, Binds to both TNFα and TNFβ (Lympho-toxin α) •Also binds to Fc portion of human IgG1 •Given s.c, 50mg a week •Pain , redness, itching & swelling at the site of injection •Chest infections increases 23
- 24. DRUGS IN GOUT
- 25. 25 Gout • Metabolic disorder characterized by hyperuricaemia • Normal plasma urate 1-6 mg/dL • Urate level over 7 in men & 6 mg/dL in women is said to be clinical hyperuricemia • Uric acid, a product of purine metabolism, has low water solubility, at low pH • When blood levels are high, it precipitates and deposits in joints, kidney and subcutaneous tissue (tophy)
- 26. 26
- 27. 27 Xanthine + Diet Adenine Guanine Hypoxanthine Uric acid Renal excretion Allantoin Probenecid Sulfinpyrazone Allopurinol Degradation Salvage HGPRT Xanthine oxidase Xanthine oxidase Uricase ATP GTP De novo synthesis Amido PRT PRPP Glutamine FIGURE49-1. Purine metabolism. Purines are synthesized via de novo syn- thesis or via the salvage pathway.The de novo pathwayutilizes the amino acid glutamine and phosphoribosyl pyrophosphate (PRPP) in a reaction catalyzed by amidophosphoribosyltrans erase (amidoPRT). In the salvage pathway, hypoxanthine-guanine phosphoribosyltrans erase (HGPRT) phosphorylates and ribosylates dietary adenine and guanine, orming the purine nucleotides (A TP and GTP) used or DNA and RNA synthesis. Degradation converts pu- rines and purine nucleotides to hypoxanthine, and xanthine oxidase converts hypoxanthine to xanthine and ultimately to uric acid, which is excreted by the kidneys or gastrointestinaltract (not shown). Pharmacologic interventions that reduce plasma urate levels include reducing urate synthesis (allopurinol and its metabolite oxypurinol), increasing urate excretion (probenecid and sul npyrazone), or converting urate to the more soluble allantoin (uricase). of IMP or guanos Nucleotide interc phosphate (ATP) a Increased activ portant consequen depletes cells of P purine synthesis. generation of mor nucleotides inhibi sulting in decrease Although purin terrelated pathwa mechanism (Fig. is deaminated, dep hypoxanthine. GM and deribosylated which is moderate xanthine is the com ther oxidation step xanthine oxidase c to xanthine and th Crosstalk betw important for ove de novo pathway rine breakdown p increases purine acid concentratio activity leads to d plasma uric acid l The importanc demonstrated by s
- 28. 28
- 29. 29 Secondary hyperuricaemia occurs in • Leukemias, lymphomas, polycythaemia • Specially when treated with chemotherapy or radiation: due to enhanced nucleic acid metabolism and uric acid production • Drug induced - thiazides, furosemide, ethacrynic acid, pyrazinamide, ethambutol, levodopa, and Clofibrate reduce uric acid excretion by kidney
- 30. 30 Drugs used for Acute Gout •NSAIDs; Indomethacin, naproxen, piroxicam phenylbutazone •Colchicine •Corticosteroids; Prednisolone
- 31. 31 Drugs for chronic gout / hyperuricaemia • Uricosurics Probenecid, Sulfinpyrazone • Synthesis inhibitor Allopurinol
- 32. 32 Acute Gout • An acute attack of gout is started by the precipitation of urate crystals in the synovial fluid • Urate crystal starts inflammatory response • Granulocyte migration into the joint; they phagocytose urate crystals and release a glycoprotein which aggravates the inflammation
- 33. 33 Acute Gout Contd… The released glycoprotein which aggravates the inflammation by • Increasing lactic acid production from inflammatory cells; local pH is reduced; more urate crystals are precipitated • Releasing lysosomal enzymes which cause joint destruction
- 34. 34 Colchicine •It is an alkaloid from Colchicum autumnale which was used in gout since 1763 •Colchicine is neither analgesic nor anti-inflammatory, •Suppresses only gouty inflammation •No effect on blood uric acid levels
- 35. 35 Colchicine Contd…. • Does not affect phagocytosis of urate crystals but inhibits release of the glycoprotein and the subsequent events • Inhibits granulocyte migration
- 36. 36 Colchicine Contd…. Other actions of colchicine are •Anti-mitotic: causes metaphase arrest by binding to microtubules, of mitotic spindle •Increases gut motility through neural mechanisms Pharmacokinetics of Colchicine •Rapidly absorbed orally; partly metabolized in liver and excreted in bile, disposal occurs in urine, faeces
- 37. 37 Colchicine Contd…. Toxicity is high and dose related •Nausea, vomiting, watery or bloody diarrhoea, abdominal cramps •Overdose produces kidney damage, CNS depression, intestinal bleeding; death is due to muscular paralysis and respiratory failure •Chronic therapy; aplastic anaemia, agranulocytosis, myopathy and loss of hair so not recommended
- 38. 38 Uses of Colchicine •Treatment of acute gout 1 mg orally followed by 0.25mg 1-3 hourly, maintenance dose 0.5-1mg/day for 4-8 weeks •Prophylaxis Colchicine 0.5-1.5 mg/day can prevent further attacks of acute gout COLCHINDQN, GOUTNIL 0.5 mg tab
- 39. 39 Corticosteroids for acute gout •Intra-articular injection of a soluble steroid suppresses symptoms effectively •In refractory cases and those not tolerating NSAIDs or Colchicine •Systemic steroids are rarely needed •Prednisolone 40-60mg may be given in one day, followed by tapering doses over few weeks
- 40. 40 CHRONIC GOUT • Pain and stiffness persist in a joint between attacks, hyperuricaemia, tophi (chalk like stone under the skin in pinna, eyelids, nose, around joints and other places) and urate stones in the kidney • Chronic gouty arthritis cause progressive disability and permanent deformities
- 41. 41 Uricosuric Drugs: Probenecid •Neither analgesic nor anti-inflammatory •Highly lipid soluble organic acid •Blocks active transport of organic acids at all sites, that in renal tubules being the most prominent
- 42. 42 Probenecid Contd…. • Penicillin + probenecid; inhibits of excretion; more sustained blood levels are achieve • Uric acid is largely reabsorbed by active transport, Probenecid, therefore, promotes excretion and reduces blood level, by inhibiting the reabsorption
- 43. 43 Pharmacokinetics of probenecid • Completely absorbed orally; 90% plasma protein bound • Partly conjugated in liver and excreted by the kidney • Plasma t1/2 is 8-10 hours Adverse effects of Probenecid • Dyspepsia is the most common side effect • Rashes, other hypersensitivity phenomena are rare • Toxic doses cause convulsions and respiratory failure
- 44. 44 Drug interactions with Probenecid • Inhibits the urinary excretion of cephalosporins, sulfonamides, methotrexate and indomethacin • Inhibits biliary excretion of Rifampicin, Pyrazinamide and ethambutol may interfere with uricosuric action of probenecid • Inhibits tubular secretion of nitrofurantoin which may not attain antibacterial concentration in urine • Salicylates block uricosuric action of probenecid
- 45. 45 Uses of Probenecid • Chronic gout: Probenecid is started at 0.25g BD and increased to 0.5g BD after a week; maximum dose 1.0 g BD • Secondary hyperuricaemia due to drugs or disease, but allopurinol is preferred • To prolong penicillin or ampicillin action by increasing and sustaining their blood levels, e.g. in gonorrhoea SABE, BENEMID, BENCID 0.5 g tab
- 46. 46 Sulfinpyrazone • Related to phenylbutazone; consistent uricosuric action • Neither analgesic nor anti-inflammatory • Inhibits tubular reabsorption of uric acid • But smaller doses can decrease urate excretion • Uricosuric action is additive with probenecid but antagonised by salicylates • Inhibits platelet aggregation and has been used for secondary prophylaxis of arterial thrombosis
- 47. 47 Sulfinpyrazone Contd…. Pharmacokinetics • Well absorbed orally; 98% plasma protein bound • Displacement interactions can occur • Uricosuric action of a single dose lasts 6 -10 hours • Inhibits metabolism of sulfonylureas and warfarin
- 48. 48 Sulfinpyrazone Contd…. Adverse effects of Sulfinpyrazone • Gastric irritation common side effect • Rashes, hypersensitivity reactions are uncommon • Unlike phenylbutazone, it does not produce fluid retention or blood dyscrasias • Start with 100 -200 mg BD, maximal dose 800 mg/day ANTURANE, ARTIRAN 200 mg cap
- 49. Uricosuric agents contd.. • Benzbromarone • MoA similar to Probenesid • Greater efficacy • Hepatotoxic • Losartan • Moderate uricosuric drug • Drug of choice in patient with concomitant hypertension 49
- 50. 50 Uric acid synthesis inhibitor: Allopurinol •Hypoxanthine analogue; Inhibitor of xanthine oxidase, responsible for uric acid synthesis •Allopurinol itself is a short acting (t ½=3 hrs) competitive inhibitor of xanthine oxidase, major metabolite alloxanthine is long acting (t1/2=24 hrs) and noncompetitive inhibitor - primarily responsible for uric acid synthesis inhibition in vivo
- 51. 51
- 52. 52 Allopurinol Contd…. Pharmacokinetics: 80% of orally absorbed; not bound to plasma proteins, metabolized largely to alloxanthine Adverse effects • Hypersensitivity; rashes, fever, malaise and muscle pain is the most frequent; Liver damage is rare • Gastric irritation, headache, nausea and dizziness
- 53. 53 Interactions with Allopurinol • Inhibits the degradation of 6-mercaptopurine and azathioprine: doses should be reduced • Potentiate warfarin and theophylline by inhibiting their metabolism • Higher incidence of skin rashes when ampicillin is given to patients on allopurinol • Iron therapy is not recommended during allopurinol treatment, the exact nature of interaction is not known, but interference with mobilization of hepatic iron stores is suggested
- 54. 54 Allopurinol Contd…. Precautions and contraindications • Excess fluid intake advised during allopurinol • Contraindications; hypersensitivity, pregnancy and lactation, elderly, children, kidney or liver disease
- 55. 55 Uses of Allopurinol • In chronic Secondary hyperuricaemia due to cancer chemotherapy /radiation /thiazides or other drugs (can even be used prophylactically in these situations) • To potentiate 6-mercaptopurine or azathioprine: in cancer chemotherapy, immunosuppressant therapy Dose: Start with 100 mg OD, maintenance dose of 300 mg/day; maximum 600 mg/day; ZYLORIC; 100, 300mg tabs; ZYLOPRIM, CIPLORIC 100 mg cap • Kala-azar: Allopurinol inhibits Leishmania by altering its purine metabolism; used as adjuvant to sodium stibogluconate in resistant cases