Download to read offline
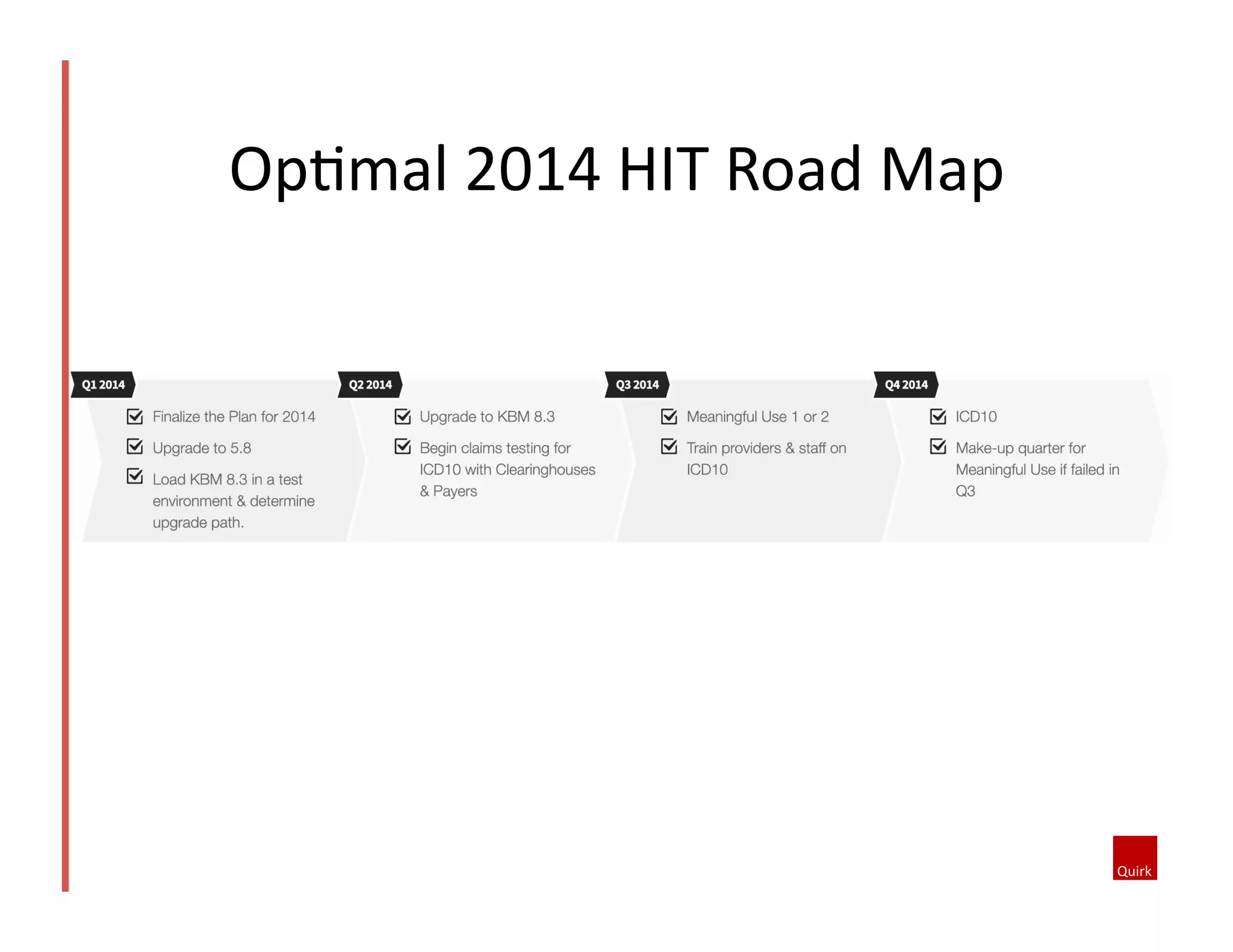
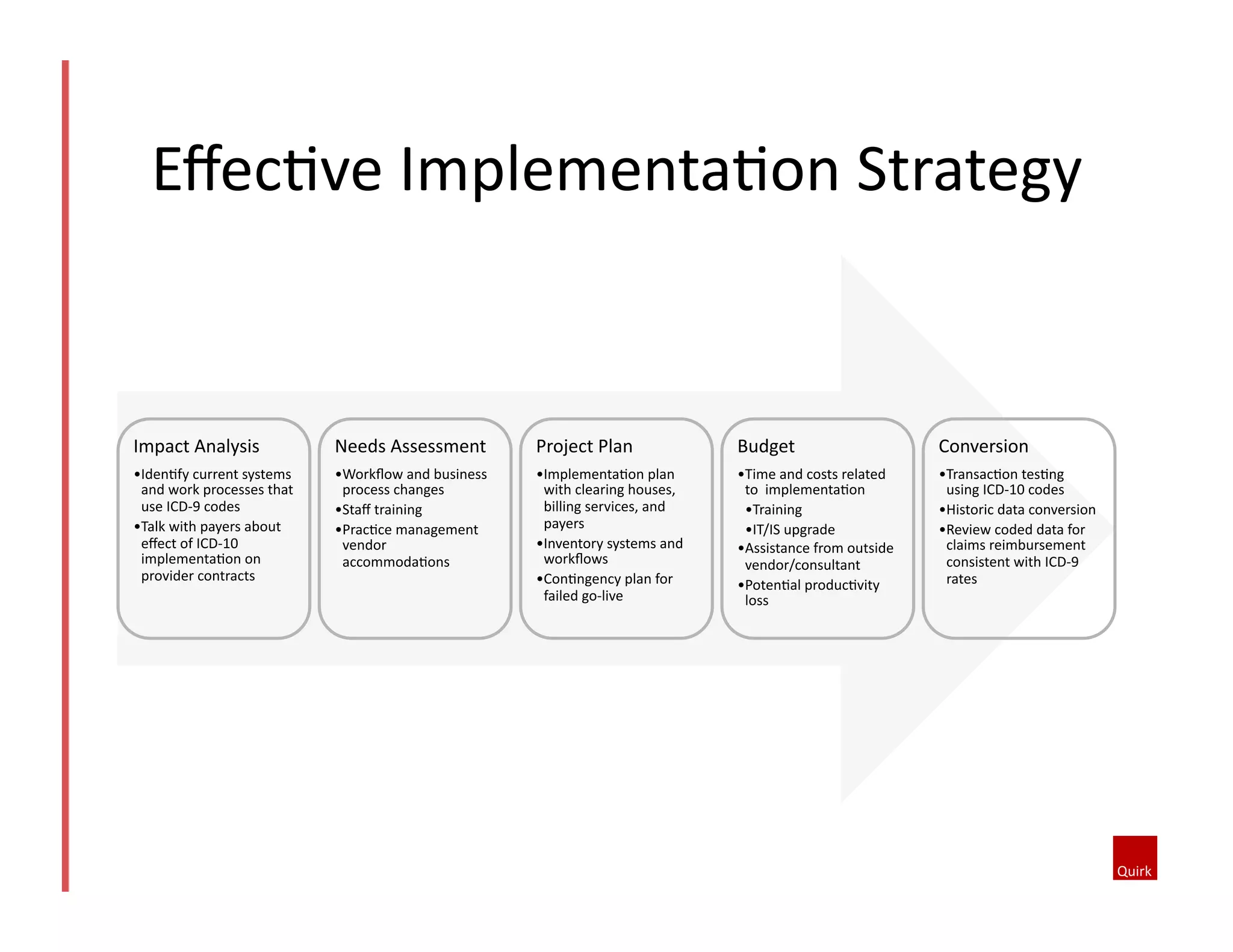
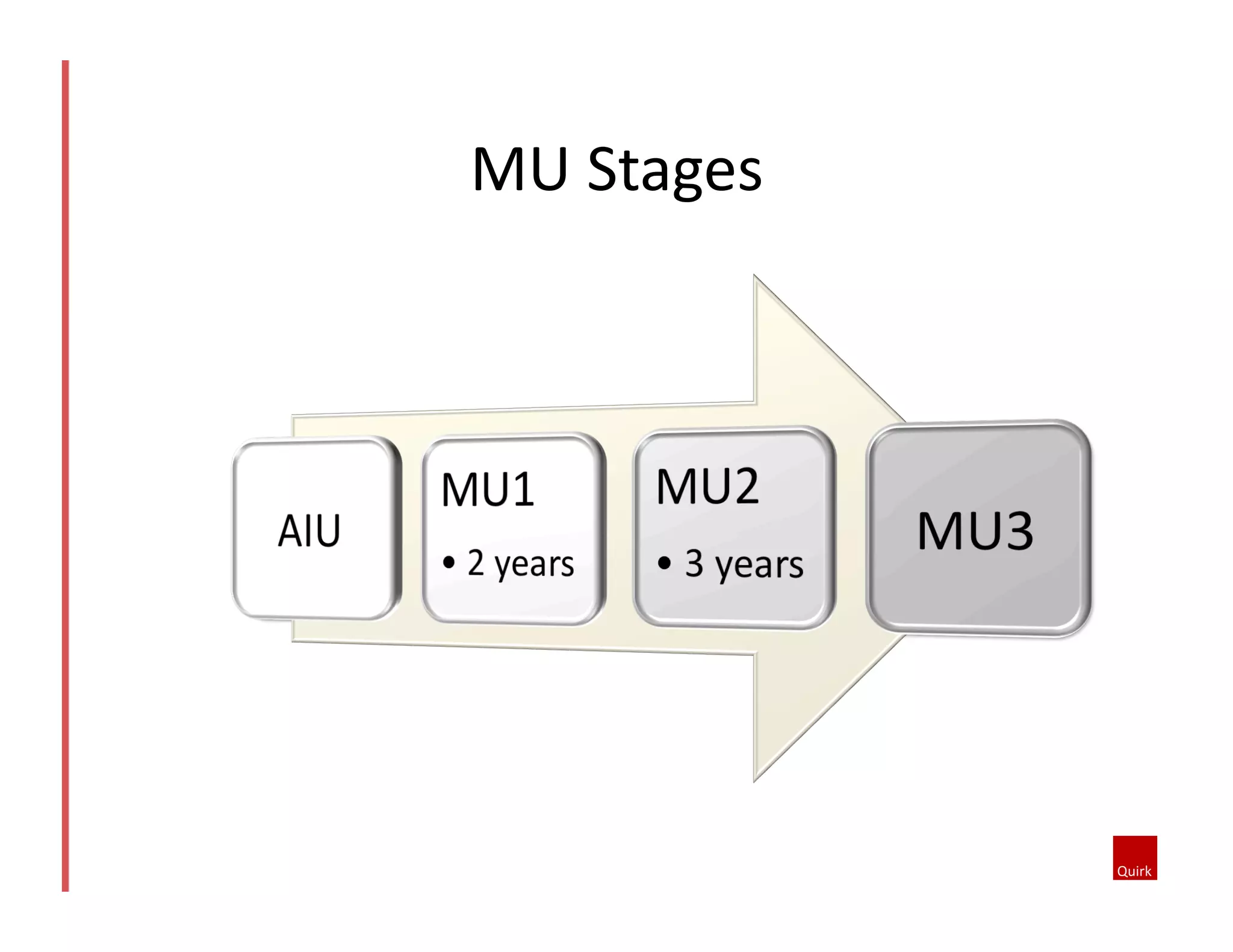

The document provides an overview of the 2014 Health IT Roadmap, outlining upgrades to NextGen and KBM systems, as well as the transition to ICD-10 coding and the implications for healthcare practices. It details the requirements for achieving Meaningful Use stages 1 and 2, the Physician Quality Reporting System (PQRS), and the Patient-Centered Medical Home (PCMH) model. Additionally, the document emphasizes the importance of training and preparation for the upcoming changes, including potential organizational impacts and the need for compliance with new regulations.






















































































