Download to read offline

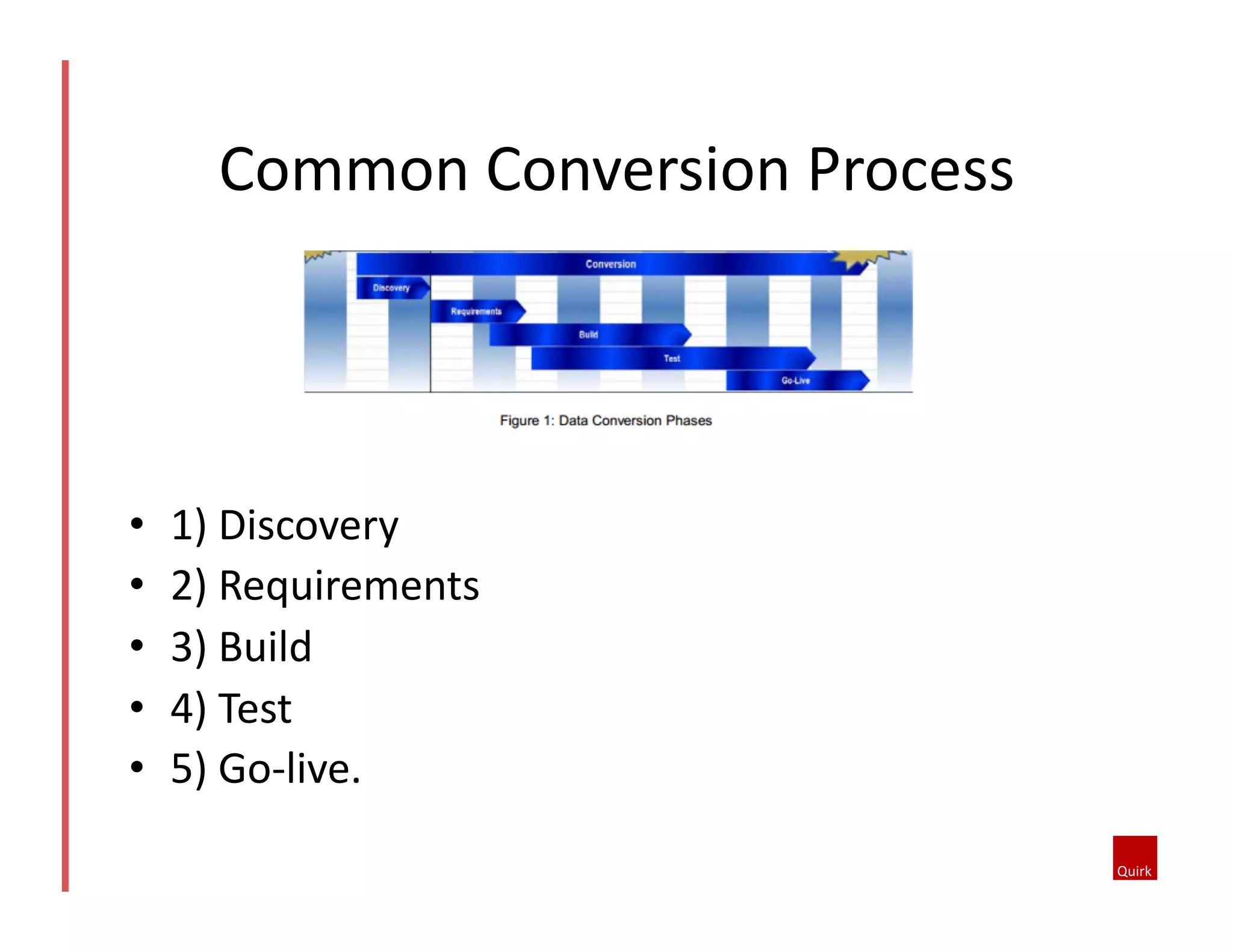

The document discusses the necessity and challenges of data conversions in healthcare systems, highlighting issues like outdated technology and improper planning. It outlines various conversion options, their pros and cons, and emphasizes the importance of a systematic approach, including stages from discovery to go-live. Key considerations include data mapping, testing, and involving clinical staff to ensure successful implementation.





























































































![Understanding Parkinson’s Disease: Causes, Symptoms, and Treatment [2025]](https://cdn.slidesharecdn.com/ss_thumbnails/understandingparkinson-251208102525-80ba3223-thumbnail.jpg?width=640&height=640&fit=bounds)



