Download as PDF, PPTX

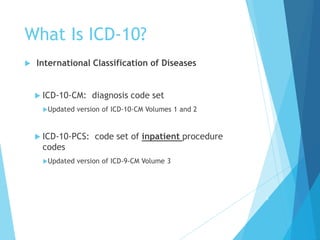
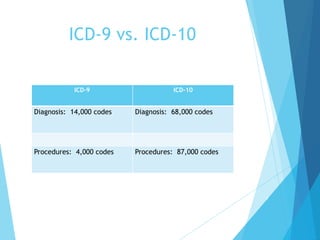
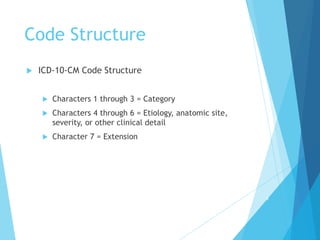
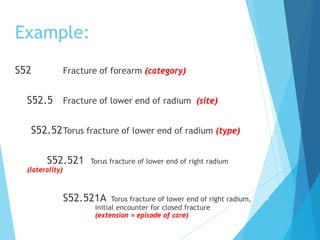









The document provides an overview and agenda for a presentation on implementing ICD-10-CM codes. The presentation covers key differences between ICD-9 and ICD-10 coding structures and requirements, impacts to various clinical and administrative areas, and tasks practices can complete to prepare for the transition. Technology considerations are also reviewed, including assessing current systems, understanding code mapping tools, and questions to ask vendors about upgrade plans and dual coding support.















































