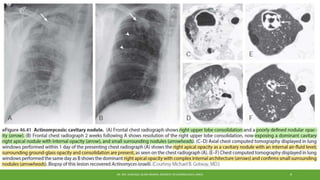
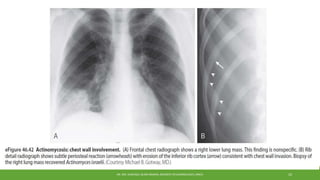
Pulmonary actinomycosis is a rare bacterial lung infection caused by Actinomyces israelii that is acquired by aspirating oropharyngeal material. It presents with chronic cough, chest pain, and sometimes hemoptysis or weight loss. Diagnosis relies on culture, biopsy showing sulfur granules, or PCR of infected tissue. Imaging often shows consolidation, nodules, or cavitary lesions confined to one lobe. Treatment is prolonged intravenous and oral penicillin, sometimes requiring surgery for complications like abscesses.