Download as PDF, PPTX




















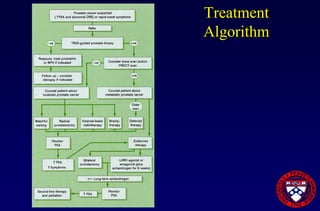


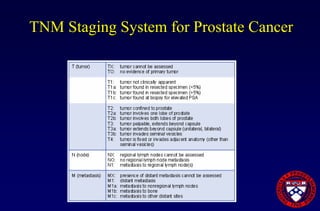






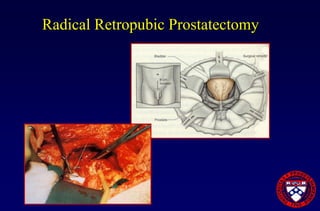

























This document provides an overview of prostate cancer, including who is affected, risk factors, detection methods like PSA testing and biopsy, staging using the Gleason score and TNM system, and treatment options like surgery, radiation therapy, active surveillance, and androgen blockade. It discusses outcomes for different treatments and challenges in managing prostate cancer recurrence after initial therapy.