This document discusses screening and biopsy for prostate cancer. It provides information on:
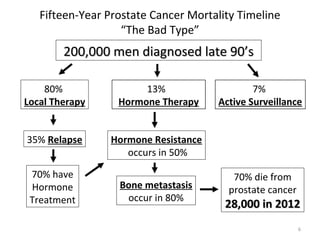
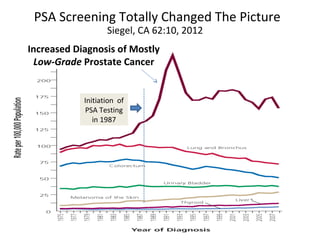
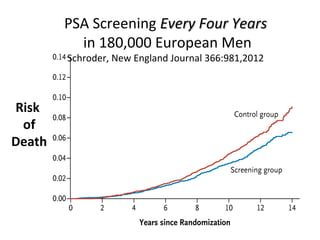
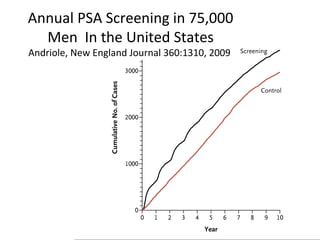
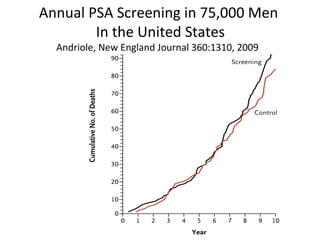
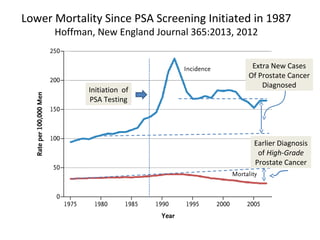
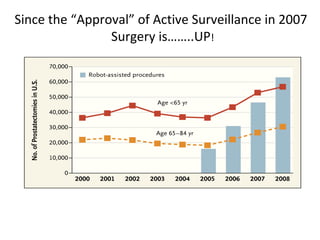
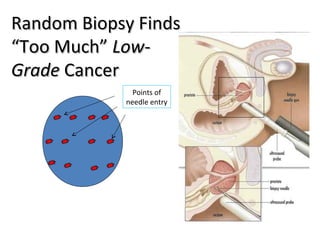
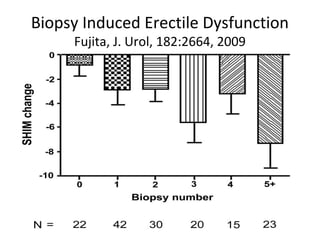
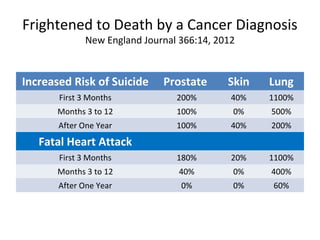
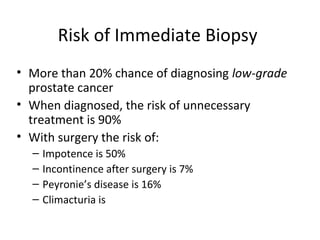
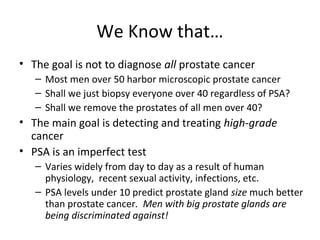
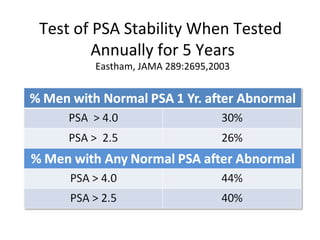
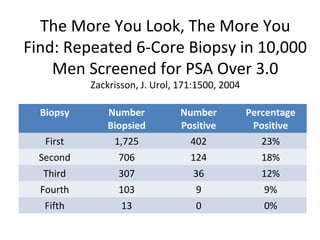
1. The imperfect nature of PSA screening and the risks of overdiagnosing low-grade prostate cancer through unnecessary biopsies and overtreatment.
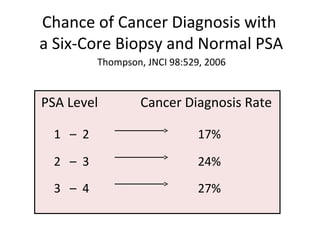
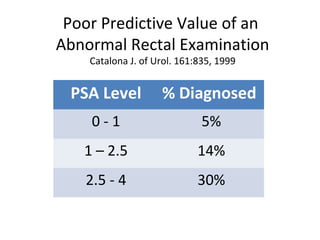
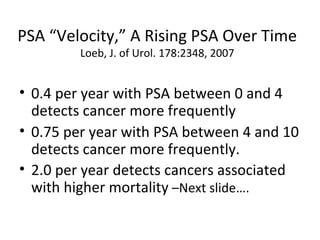
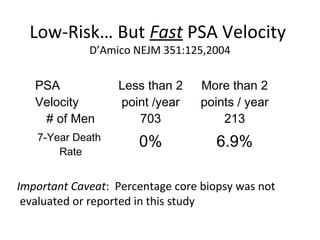
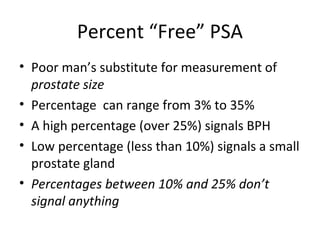
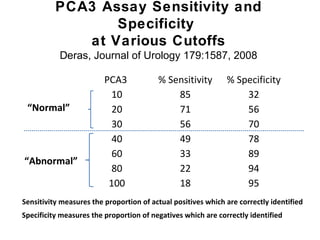
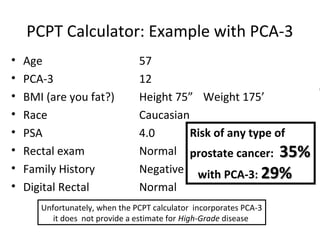
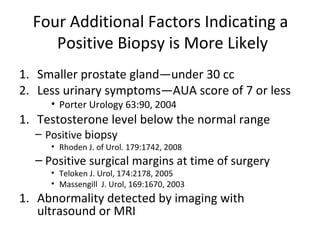
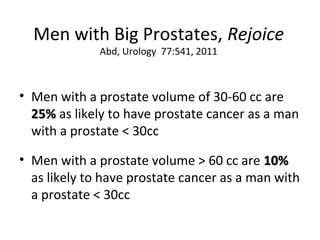
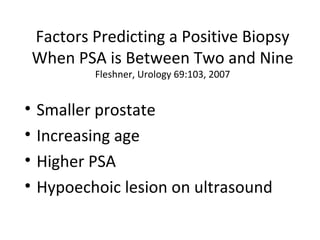
2. Factors that can help determine the likelihood of finding cancer on biopsy for men with elevated PSA levels, such as prostate size, family history, and PCA3 urine tests.
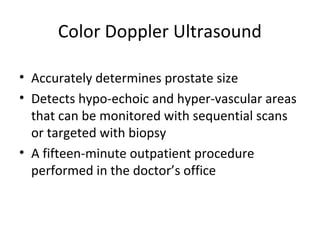
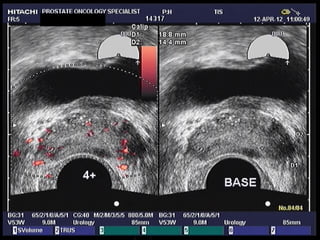
3. Imaging options like MRI that may improve accuracy and allow targeted biopsies to avoid unnecessary procedures.