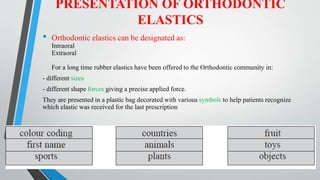
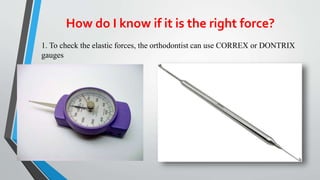
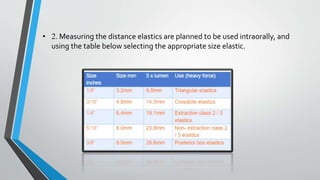
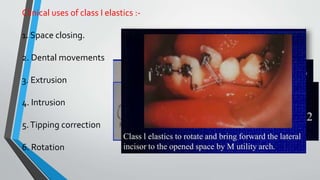
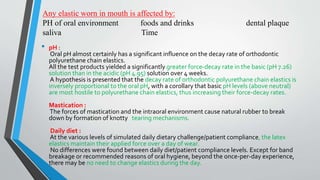
This document discusses various types of orthodontic elastics, including their properties, uses, and effects. It describes intraoral and extraoral elastics and notes they come in different sizes and forces. Key elastic types summarized are:
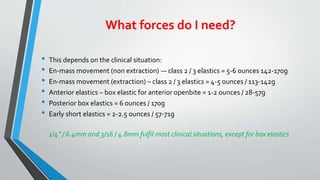
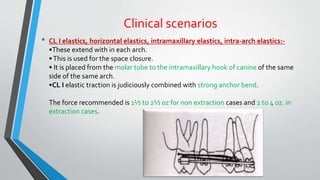
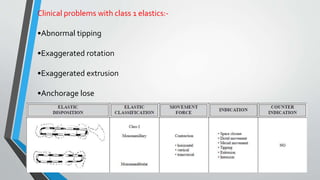
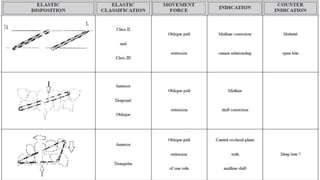
- Class I elastics used for space closure within each arch. Forces range from 1.5-2.5oz for non-extraction and 2-4oz for extraction cases.
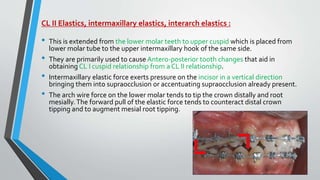
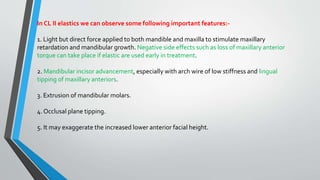
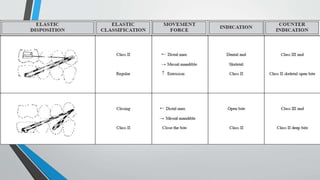
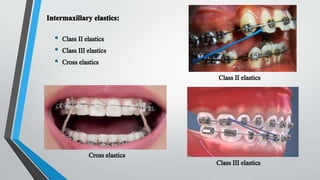
- Class II elastics extend from lower molars to upper cuspids to correct malocclusions. Forces are 5-6oz and 4-5oz respectively.
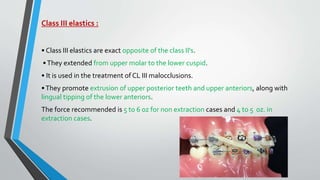
- Class III elastics do the opposite, extending from upper molars to lower cuspids. Forces are also



![Properties:
Visco elasticity
Creep [stress – relaxation]
Hysteresis
Hysteresis loss](https://image.slidesharecdn.com/elastics-240221220245-33c7869c/85/Proper-_-Elastics-_-in-_-orthontics-pptx-5-320.jpg)
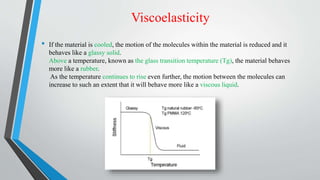
![Creep [stress – relaxation]
• This is the time dependant permanent deformation that occurs when the
material is subjected to a constant load.](https://image.slidesharecdn.com/elastics-240221220245-33c7869c/85/Proper-_-Elastics-_-in-_-orthontics-pptx-7-320.jpg)



























![Loops in orthodontics and its uses [Autosaved]..ppt](https://cdn.slidesharecdn.com/ss_thumbnails/loopsinorthodonticsautosaved-241204161830-0e1eccec-thumbnail.jpg?width=640&height=640&fit=bounds)













































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














