Downloaded 56 times



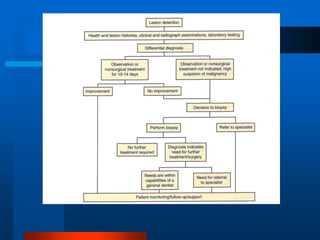

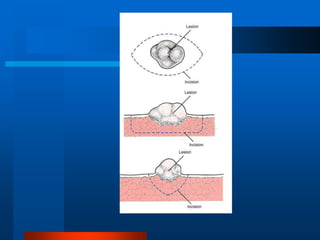
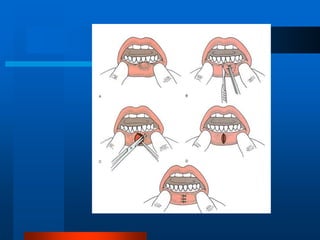
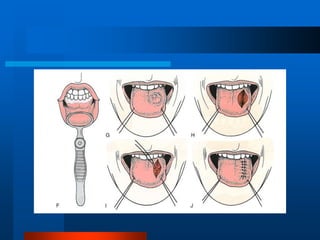
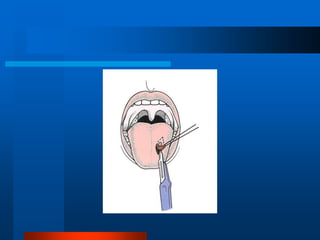
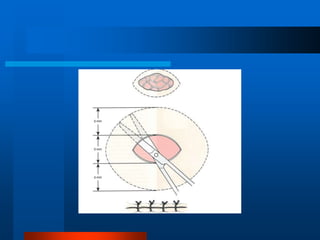

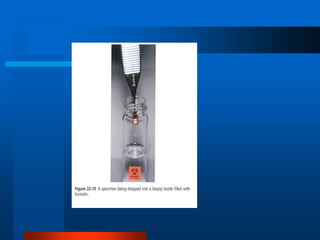

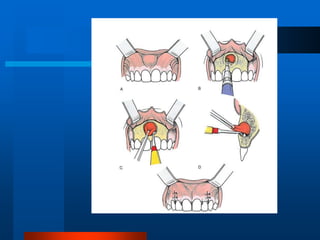


This document discusses principles and techniques of biopsy. It outlines the steps involved in evaluating a patient with an oral lesion including taking a health history, examining the lesion history, performing a clinical and radiographic exam, and potentially obtaining laboratory tests. It describes different types of biopsies including incisional, excisional, and intraosseous biopsies. Principles of biopsy such as anesthesia, hemostasis, handling specimens, and closure techniques are also outlined. The goal is to obtain sufficient tissue for accurate histopathologic evaluation.





































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




