Downloaded 1,279 times
![Biopsy [BIO =LIFE
OPSIS=VISION]
Biopsy is the removal of the tissueremoval of the tissue from
the living organism for the purpose of
histopathological examinationhistopathological examination and
diagnosis.
A biopsy is the examination of tissueexamination of tissue
removed from a lesion and by extension
the term is also used to convey the
removal of the tissue.[WHO 1966]](https://image.slidesharecdn.com/biopsy-160630130928/85/Biopsy-2-320.jpg)
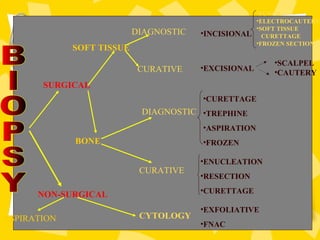


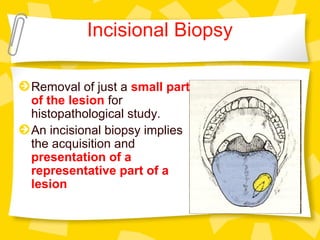



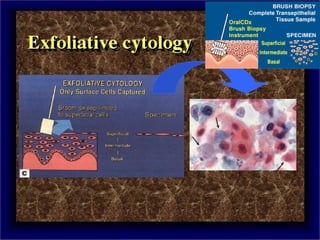
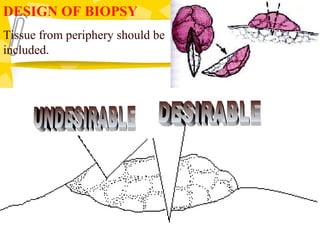





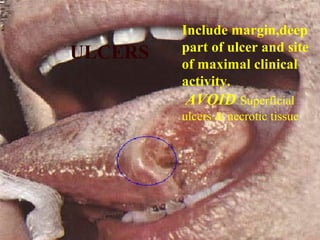


Biopsy is the removal and examination of tissue to diagnose a condition. It can be excisional, removing the entire lesion, or incisional, removing part of a lesion. Indications include persistent lesions without a clear cause, suspected tumors or malignancies, and lesions interfering with function. Contraindications are poor health and acute infection. Types include punch, frozen section, aspiration, and exfoliative cytology. Care must be taken in design, handling, and potential dangers like spreading or infection. Biopsy provides diagnostic and treatment guidance.























































































