Downloaded 1,715 times

















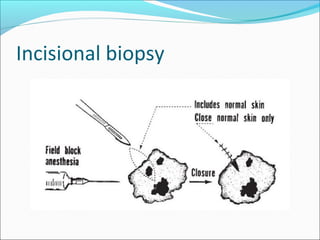






























A biopsy is a surgical procedure to obtain tissue samples for microscopic examination and diagnosis. The main types of biopsies are cytology, aspiration, incisional, and excisional. Cytology examines individual cells but cannot provide histologic details, while aspiration uses a needle to remove fluid or cells. Incisional biopsies remove a portion of tissue, while excisional biopsies completely remove small lesions. Proper biopsy techniques aim to obtain representative tissue samples while avoiding thermal or mechanical damage. Careful documentation and handling of specimens aids pathological examination and diagnosis.



































































