Download as PDF, PPTX





















![ US PREVENTIVE SERVICES TASK FORCE [under revision]
o MEN:
• Strongly recommends screening men aged ≥35 years for lipid
disorders.
• Recommends screening men aged 20-35 for lipid disorders if they are
at increased risk for CHD.
o WOMEN:
• Strongly recommends screening women aged ≥45 years for lipid
disorders if they are at increased risk for CHD.
• Recommends screening women aged 20-45 for lipid disorders if they
are at increased risk for CHD.
HEDIS
o Required for 18 to 75 y/o discharged after AMI or CABG or any
percutaneous coronary intervention during the last two (2) years.
o LDL-C yearly (<100 mg/dL) [last value on record within the last year]](https://image.slidesharecdn.com/primarycarescreeningtestsinadultsgeriatrics-160126171846/75/Primary-care-screening-tests-in-adults-geriatrics-28-2048.jpg)




![ Examples of an advance care plan
o Advance directive: Directive about treatment preferences and the
designation of a surrogate who can make medical decisions for a
patient who is unable to make them (e.g., living will, power of
attorney, health care proxy).
o Actionable medical orders: Written instructions regarding initiating,
continuing, withholding or withdrawing specific forms of life-
sustaining treatment (e.g., Physician Orders for Life Sustaining
Treatment [POLST]).
o Living will: Legal document denoting preferences for life-sustaining
treatment and end-of-life care.
o Surrogate decision maker: A written document designating
someone other than the member to make future medical treatment
choices.](https://image.slidesharecdn.com/primarycarescreeningtestsinadultsgeriatrics-160126171846/75/Primary-care-screening-tests-in-adults-geriatrics-36-2048.jpg)
![ Documentation in the medical record must include evidence of a complete
functional status assessment and the date when it was performed.
Notations for a complete functional status assessment must include one of
the following:
o Notation that Activities of Daily Living (ADL) were assessed or that at least five of the
following were assessed: bathing, dressing, eating, transferring [e.g., getting in and
out of chairs], using toilet, walking.
o Notation that Instrumental Activities of Daily Living (IADL) were assessed or at least
four of the following were assessed: shopping for groceries, driving or using public
transportation, using the telephone, meal preparation, housework, home repair,
laundry, taking medications, handling finances.
o Result of assessment using a standardized functional status assessment tool.
o Notation that at least three of the following four components were assessed:
• Cognitive status.
• Ambulation status.
• Hearing, vision and speech (i.e., sensory ability).
• Other functional independence (e.g., exercise, ability to perform job).](https://image.slidesharecdn.com/primarycarescreeningtestsinadultsgeriatrics-160126171846/75/Primary-care-screening-tests-in-adults-geriatrics-38-2048.jpg)



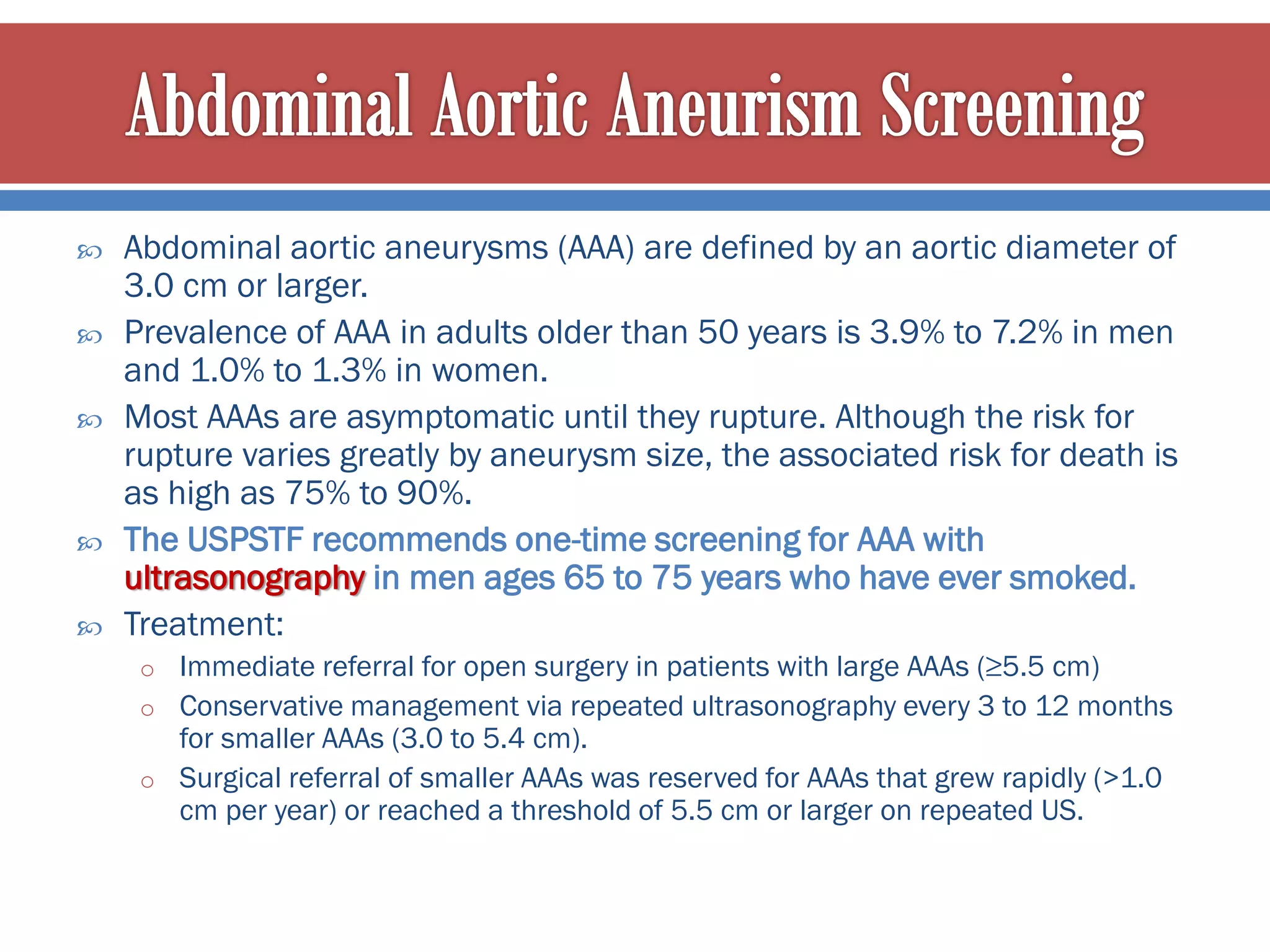


The document summarizes guidelines for preventive health screenings from organizations like the US Preventive Services Task Force. It discusses screening recommendations for conditions like high blood pressure, obesity, breast cancer, cervical cancer, sexually transmitted infections, hepatitis C, colorectal cancer, and lipid disorders. The recommendations include screening age ranges and time intervals, accepted screening tests, and risk factors to consider for more frequent screening. The document emphasizes the importance of early preventive interventions to decrease mortality rates from leading causes of death.