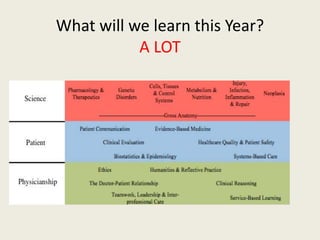
This document outlines the learning objectives and topics covered in an introductory clinical medicine course. The objectives are to develop knowledge of medical ethics and professionalism, clinical skills like self-care and reflecting on experiences, and attitudes like patient-centered care. Key topics include physicianship skills like communication and medical interviewing, the patient-physician relationship, professionalism, the life cycle, chronic illness, and cultural competence. Various teaching methods like lectures, role-playing, patient interviews, and video clips will be used.






























![Kemahiran hidup bersepadu led [light emitting diode]](https://cdn.slidesharecdn.com/ss_thumbnails/kemahiranhidupbersepadu-140917022022-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)






![Y Murphy Dr Pt Comm Curriculum 2010 AACH Forum[1]](https://cdn.slidesharecdn.com/ss_thumbnails/2010drptcommintroslidesaach1-101014083021-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


































