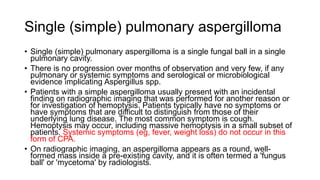
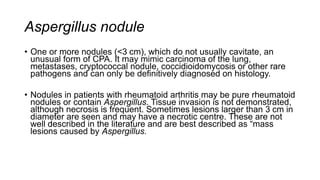
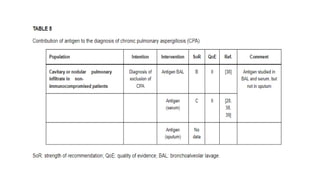
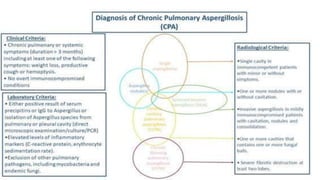
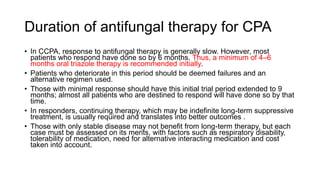
Chronic pulmonary aspergillosis (CPA) is a long-term lung infection primarily caused by Aspergillus fumigatus, affecting individuals with a history of structural lung diseases like tuberculosis and COPD. The disease can present in various forms, including simple aspergilloma and chronic cavitary pulmonary aspergillosis, and is characterized by the local immune response to fungal colonization rather than extensive tissue invasion. Diagnosis involves imaging findings, serological tests, and exclusion of alternative diagnoses, with diverse symptoms ranging from chronic cough to hemoptysis.

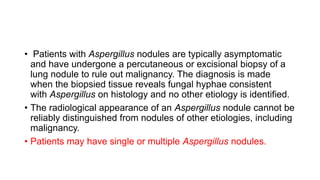
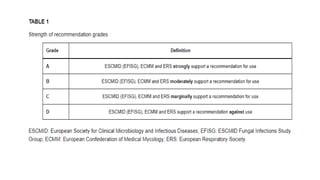
![• Mild to moderate immunocompromise (eg, low-dose corticosteroids [eg, <
equivalent of prednisone 0.3 mg/kg/day for >3 weeks]) predisposes to a specific
form of CPA called subacute invasive aspergillosis (SAIA).
• Other conditions, including bronchiectasis, prior pneumothorax, COVID-19
infection, prior severe pneumonia, pneumoconiosis, silicosis, rheumatoid arthritis,
ankylosing spondylitis, granulomatosis with polyangiitis, previous pulmonary
embolism, and hydatid disease.
• Aspergillus fumigatus (A. fumigatus) is the most common cause of CPA,
although A. flavus, A. niger, A. terreus, and A. nidulans have also been implicated.](https://image.slidesharecdn.com/chronicpulmonaryaspergillosis-240707152508-2918e3c9/85/Presentation-on-Chronic-Pulmonary-Aspergillosis-4-320.jpg)
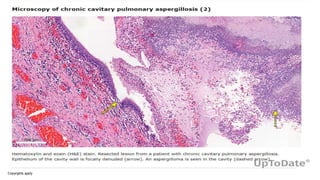
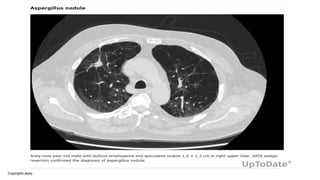
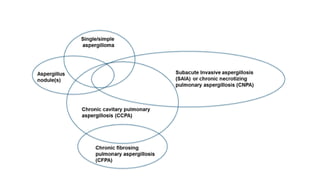
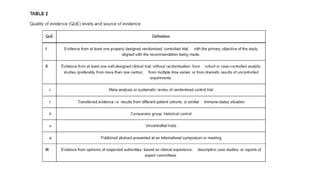
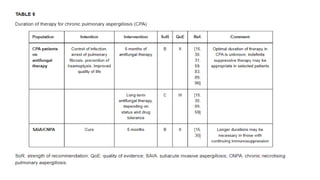
![• Two additional forms of CPA are due to extensive tissue
inflammation in response to Aspergillus colonization of
previously damaged lungs. Actual fungal organisms are
uncommonly found in affected lung tissue:
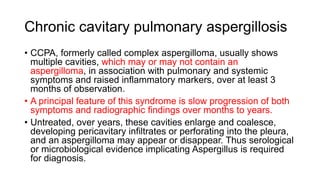
1. Chronic cavitary pulmonary aspergillosis (CCPA) [Most
common type]
2. Chronic fibrosing pulmonary aspergillosis (CFPA)
• Subacute invasive aspergillosis (SAIA)](https://image.slidesharecdn.com/chronicpulmonaryaspergillosis-240707152508-2918e3c9/85/Presentation-on-Chronic-Pulmonary-Aspergillosis-7-320.jpg)


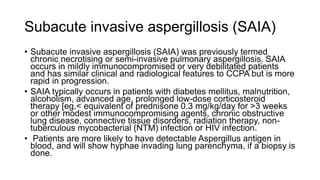


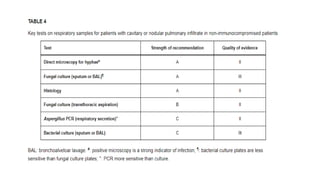
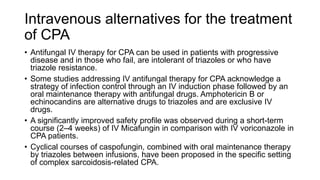
![Laboratory findings
• Routine laboratory tests in patients with CPA often reflect the
presence of chronic inflammation, with anemia of chronic
disease, lymphopenia, hypoalbuminemia, elevated
inflammatory markers (erythrocyte sedimentation rate [ESR]
and C-reactive protein), and polyclonal
hypergammaglobulinemia.
• Laboratory findings are usually normal in patients with simple
aspergillomas or Aspergillus nodules.](https://image.slidesharecdn.com/chronicpulmonaryaspergillosis-240707152508-2918e3c9/85/Presentation-on-Chronic-Pulmonary-Aspergillosis-34-320.jpg)
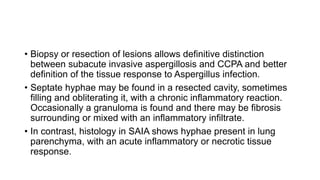

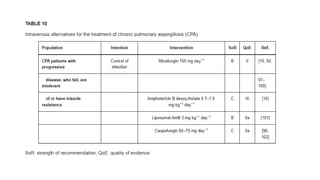
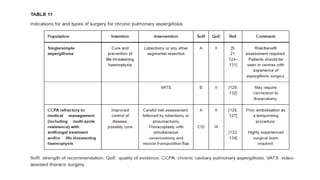
![Indications for surgery in CPA
• Surgical resection of aspergilloma is a definitive treatment option for patients with adequate pulmonary function.
• Success of the procedure depends on the ability to fully resect the aspergilloma without spillage of fungal elements into
the pleural space.
• As such, recurrence of disease and haemoptysis are rare in simple aspergilloma while CCPA carries a lower success
rate.
• Surgery should be considered in all patients with severe haemoptysis.
• Prior to possible elective surgery, careful patient selection [125] is warranted as many patients are physically debilitated
contributing to a higher risk of death and peri- and post-operative complications. In this regard special emphasis should
be given to cardiopulmonary function.
• Malnourished patients should have supplemental feeding to improve nutritional status before surgery, including the use
of nasogastric or percutaneous endoscopic gastrostomy feeding if oral supplementation is inadequate.
• In patients not deemed candidates for surgery because of a high risk profile, bronchoscopic removal of the aspergilloma
should be considered.
• Risk of peri- or post-operative complications and mortality are significantly higher in patients with multi-cavity disease
(CCPA) compared with simple aspergilloma.
• Procedures include bullectomy, segmentectomy, sublobar resection, wedge resection, lobectomy, pleurectomy,
pneumonectomy. Video-assisted thoracic surgery (VATS) may reduce the number of complications and length of
hospitalisation and has been suggested as an alternative procedure to open surgery for the resection of simple
aspergilloma and multicavity disease without infiltration of the hilum](https://image.slidesharecdn.com/chronicpulmonaryaspergillosis-240707152508-2918e3c9/85/Presentation-on-Chronic-Pulmonary-Aspergillosis-72-320.jpg)








![Interstitial Lung Diseases [ILD] Approach to Management](https://cdn.slidesharecdn.com/ss_thumbnails/interstitiallungdiseases-arunvasireddy-19october2015-seminar-171016041856-thumbnail.jpg?width=640&height=640&fit=bounds)


































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

