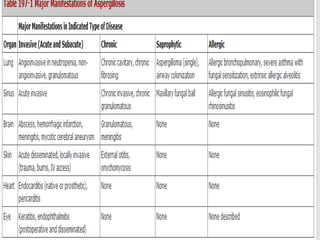
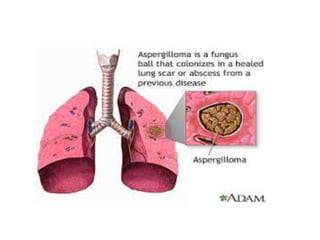
This document provides an overview of pulmonary aspergillosis, caused by inhalation of the fungus Aspergillus. It discusses the main types including aspergilloma (fungal ball in a pre-existing lung cavity), allergic bronchopulmonary aspergillosis (ABPA, an immune response in people with asthma or cystic fibrosis), and invasive aspergillosis which occurs in immunocompromised people. The pathology, risk factors, clinical features, diagnosis and treatment are described for each type. ABPA is characterized by severe asthma attacks, mucus plugs and bronchial obstruction visible on chest imaging.

![Pulmonary aspergillosis
Primarily affects the lungs, causing the following
main syndromes:
• Allergic bronchopulmonary aspergillosis (ABPA)
• Invasive aspergillosis
• Chronic necrotizing Aspergillus pneumonia (or
chronic necrotizing pulmonary aspergillosis
[CNPA])
• Aspergilloma](https://image.slidesharecdn.com/aspergillosisandthelungs2-150509193751-lva1-app6892/85/Aspergillosis-and-the-lungs-Dr-Adetunji-T-A-12-320.jpg)
![References
• Harrison’s Principles Of Int Med 18th ed
• 1.Joshi JM. Hydatidothorax. Lung India 2011;28:315-6. Back to cited text no.
1 [PUBMED]
• 2.Biswas D, Dey A, Biswas S, Chakraborty M. It's easy to miss complicated hydatid
cyst of lung. Lung India 2010;27:164-6. Back to cited text no. 2 [PUBMED]
• 3.Sarkar SK, Kumar V, Sharma SD, Bhatnagar M, Khandelwal PP. Crescent sign in
pulmonary hydatid cyst. Lung India 1988;6:155-6. Back to cited text no. 3
• 4.Flisser A. Larval cestodes. In: Collier L, Balows A, Sussman M, editors. Topley and
Wilson's microbiology and microbial infections. Parasitology. 9 th ed. Vol. 5. New
York, NY: Oxford University Press; 1998. p. 539-60. Back to cited text no. 4
• 5.Ulkü R, Yilmaz HG, Onat S, Ozçelik C. Surgical treatment of pulmonary hydatid
cysts: Report of 139 cases. Int Surg 2006;91:77-81. Back to cited text no. 5
• 6.Sharif A, Ansarin K, Rashidi F, Taghizadieh A. Bronchoscopic diagnosis and
removal of a ruptured hydatid cyst. J Bronchology Interv Pulmonol 2011;18:362-4.
• Holding KJ et al Aspergillosis Among People Infected with Human
Immunodeficiency Virus; Incidence And Survival, Adult and Adolescents Spectrum
of HIV Disease Project Clin Infect Dis 2000;31:1253](https://image.slidesharecdn.com/aspergillosisandthelungs2-150509193751-lva1-app6892/85/Aspergillosis-and-the-lungs-Dr-Adetunji-T-A-46-320.jpg)



































































