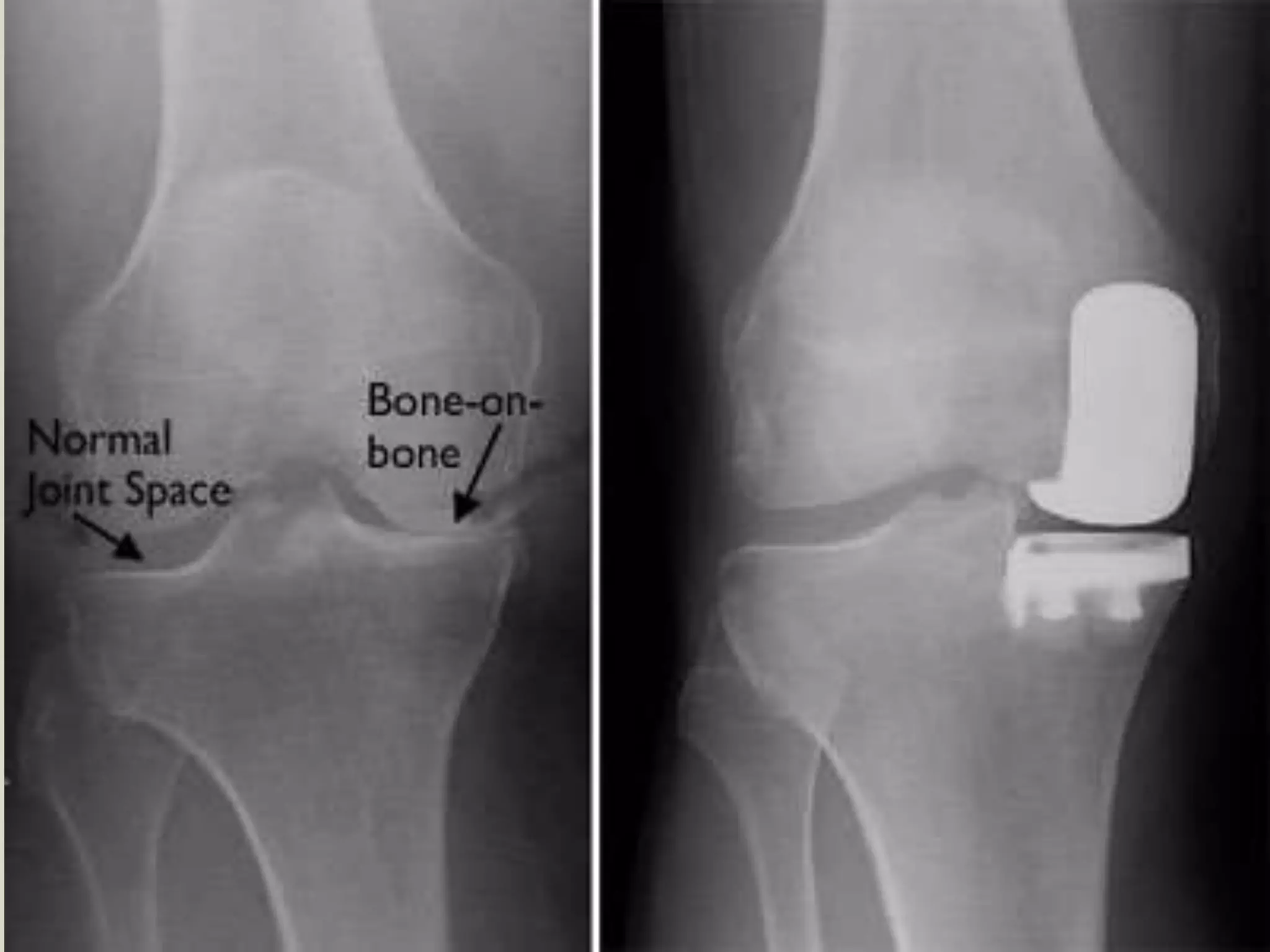
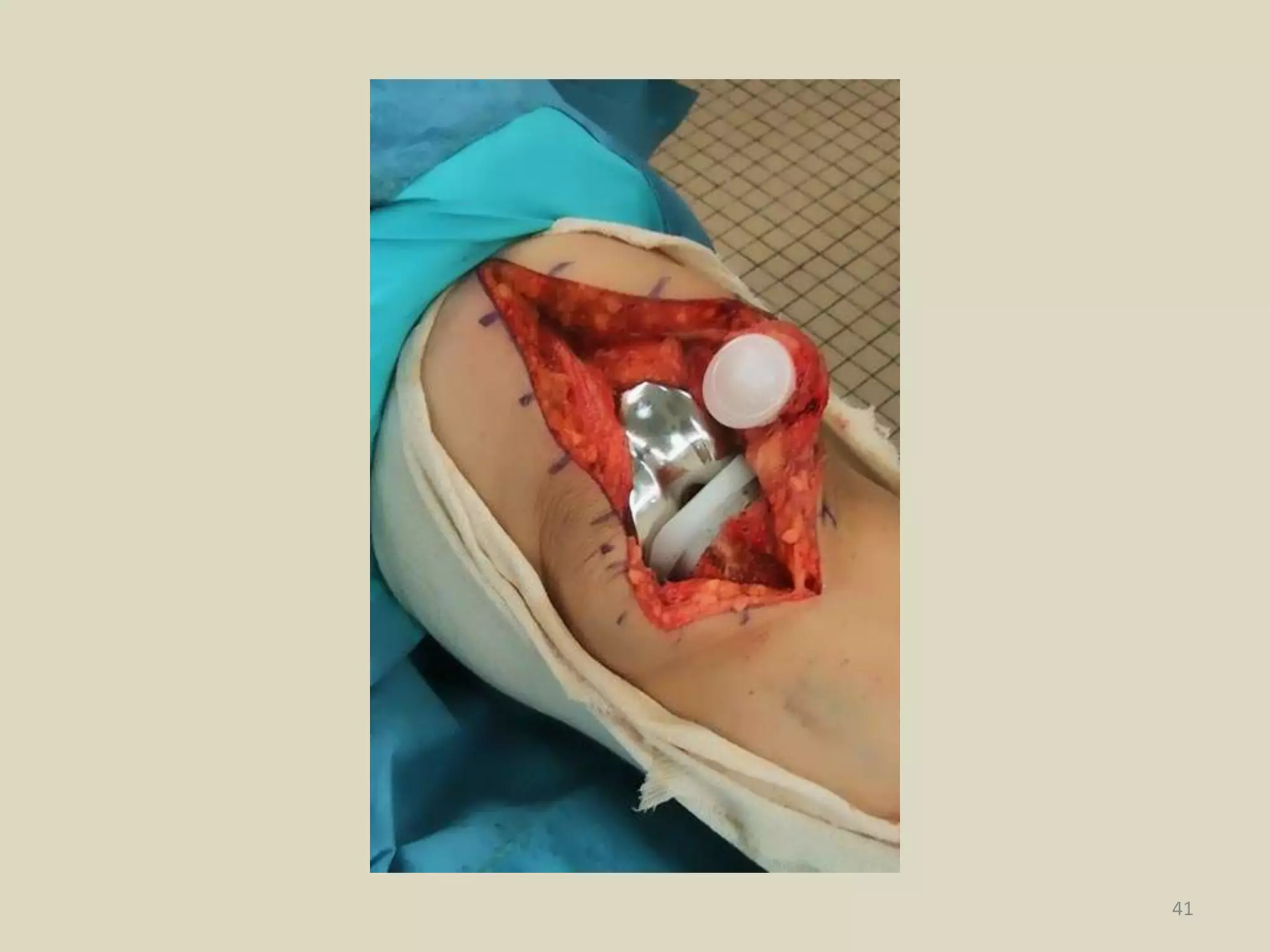
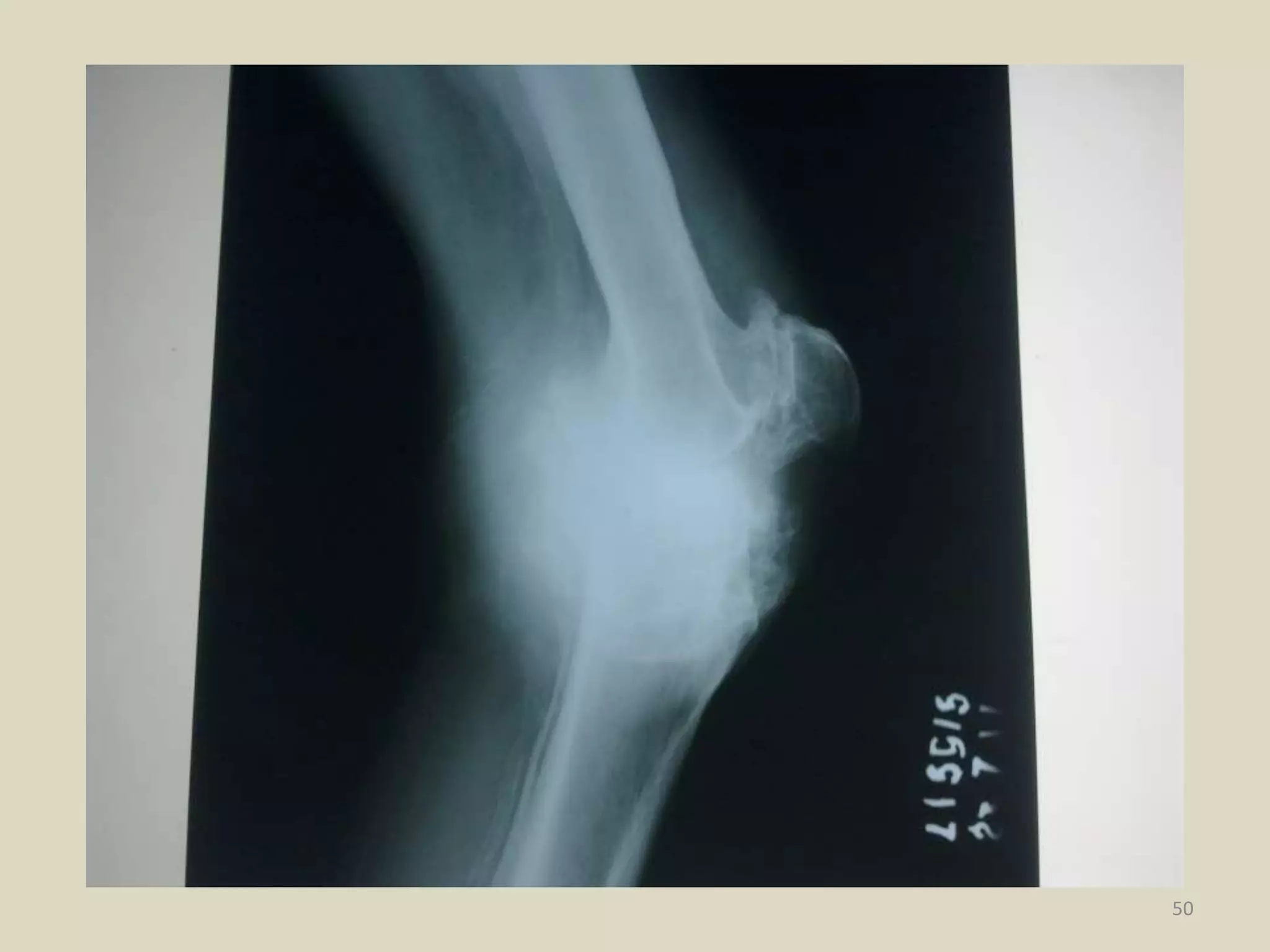
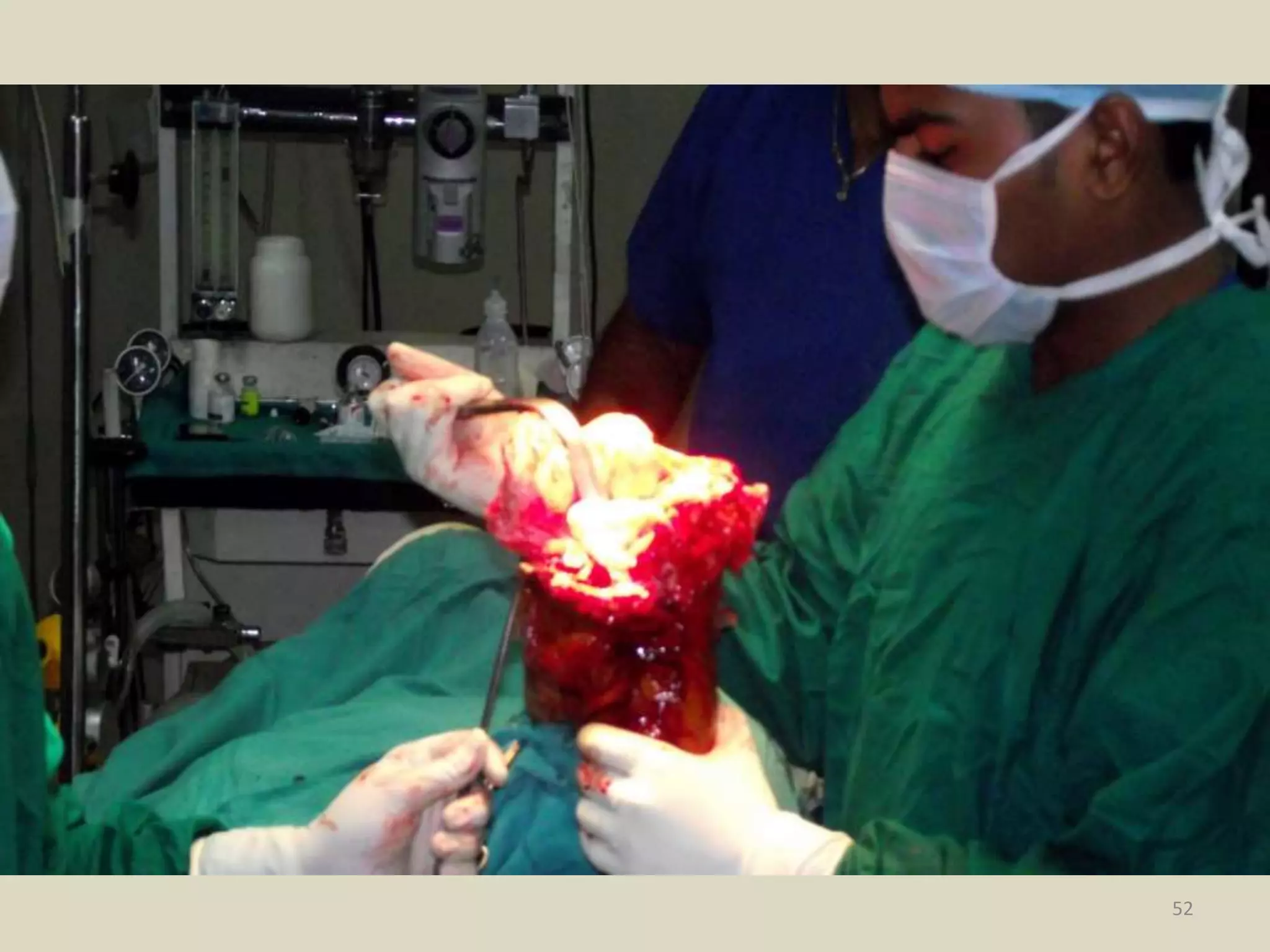
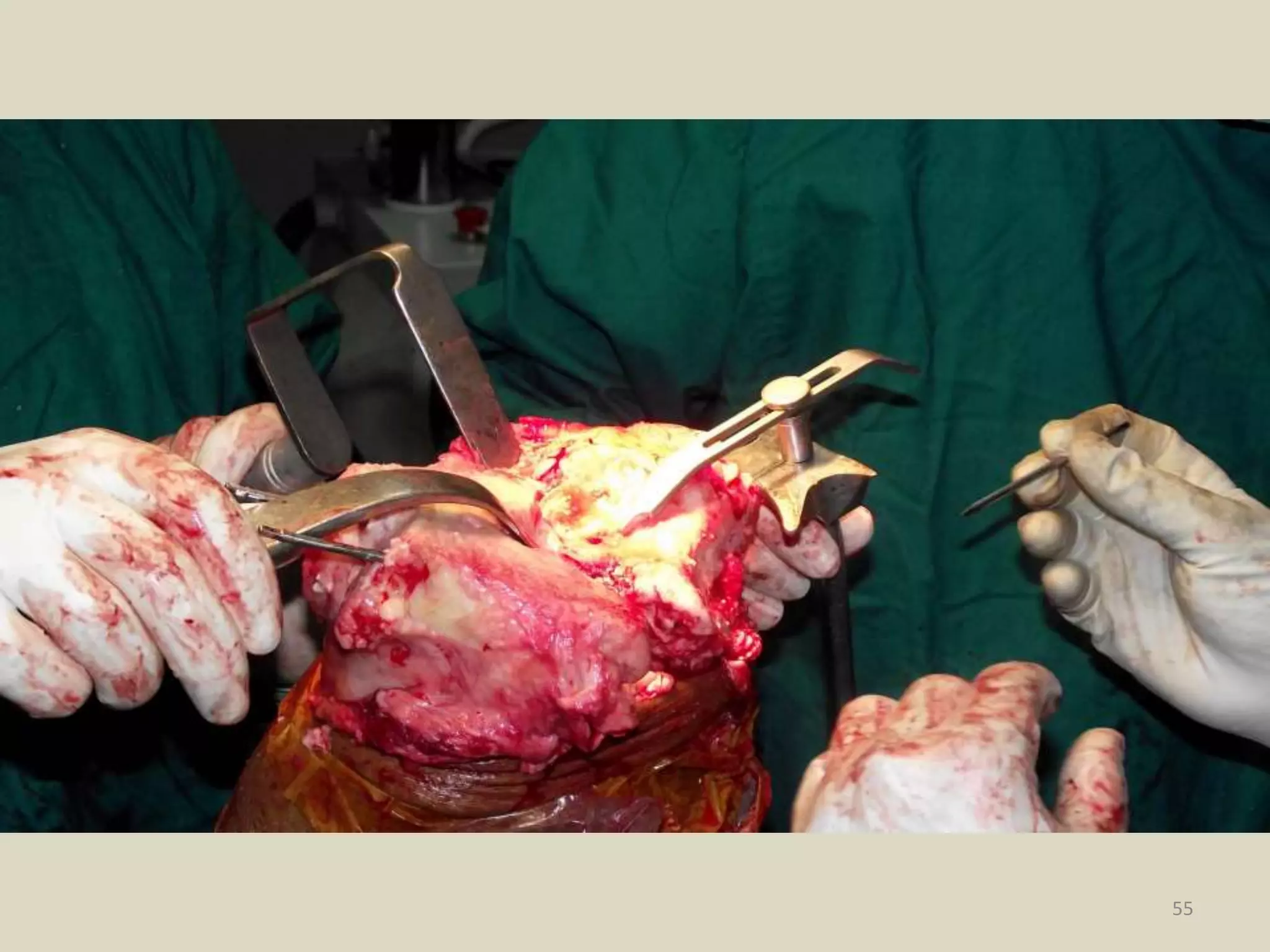
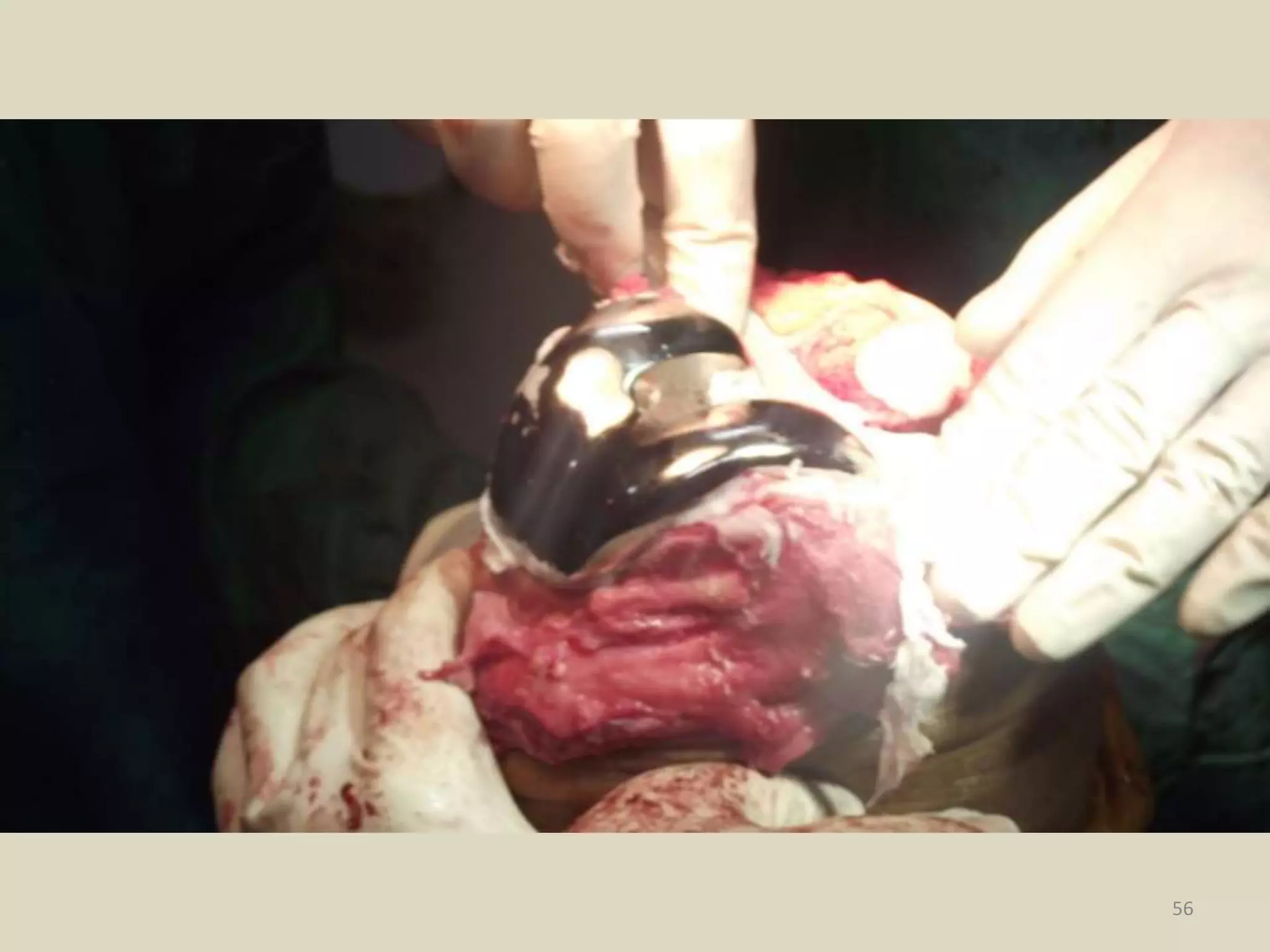
Osteoarthritis is a degenerative joint disease involving the entire joint, including cartilage, bone and synovium. It commonly affects the knees and presents with joint pain and stiffness that worsens with use. Treatment focuses on reducing pain and improving function through non-pharmacological means like exercise and weight loss as well as drugs. For knees, management may include injections, hyaluronic acid, glucosamine, NSAIDs, opioids and surgery ranging from arthroscopy to partial or total knee replacement in advanced cases. The goals are long-term pain relief and functional restoration through a multimodal approach.