
Downloaded 128 times


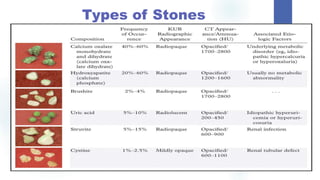
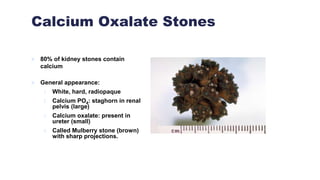
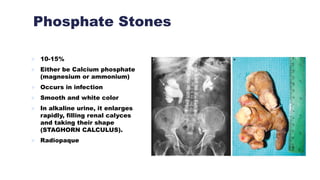
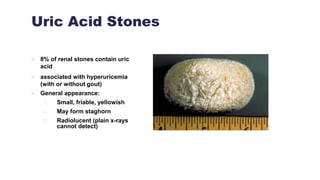




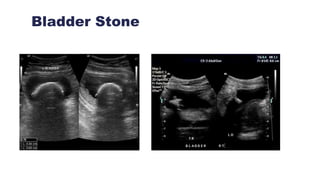



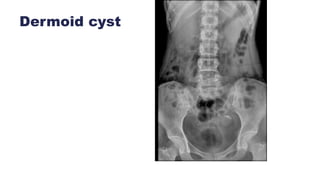
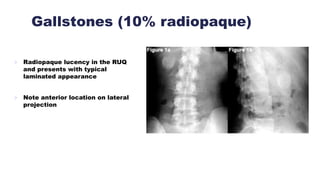
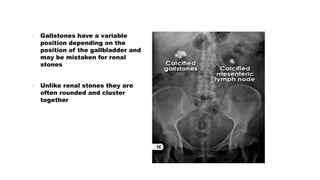
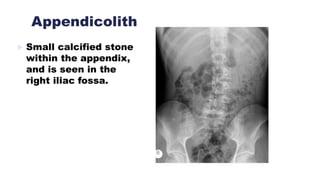
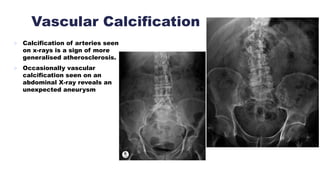
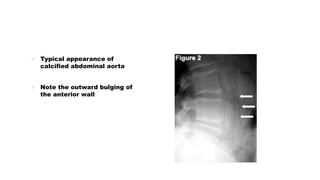




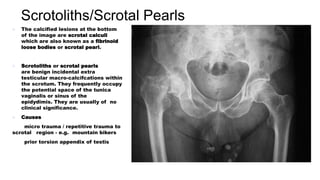

This document discusses different types of stones that can form in the urinary tract, including calcium oxalate, phosphate, uric acid, and struvite stones. It also discusses conditions that can mimic stones on imaging, such as nephrocalcinosis, phleboliths, pancreatic and adrenal calcification, dermoid cysts, gallstones, and vascular and renal calcification. Stones can cause obstruction of the urinary tract and lead to hydronephrosis. Specific stone locations like ureteric, bladder, and jack stones are also covered.























































































