Downloaded 40 times







![Midstream Interventions,
cont.
Housing(1 study) – all households received helpful housing
modifications, with decreased hospital admissions for those up to 34
years old, decreased housing-related, preventable hospital
admissions.
Social & Physical Environments (3 studies) -
Eight projects resulting from a collaborative demonstrated organizational change and
advocacy projects at multiple levels, but had no impact on program integration or policy
School-based break time snacking reduced indicators of childhood dental disease (DMFT
changed from 1.13, CI [0.85, 1.40] in year 1 to 1.58, CI [1.28, 1.89] in year 2) and
increased number of filled permanent teeth in lower SES schools over time: mean 0.49,
CI [0.20, 0.77] Year 1 and 1.05, CI [0.69, 1.14] Year 2.
Chronic disease coalition did not report health outcomes but initiated a
number of programs, policies, and practices with outcomes not yet available](https://image.slidesharecdn.com/pp28intersectoralcollaborationwebinar19-sept-2012-120920130655-phpapp01/75/Intersectoral-Action-the-Social-Determinants-of-Health-What-s-the-Evidence-23-2048.jpg)
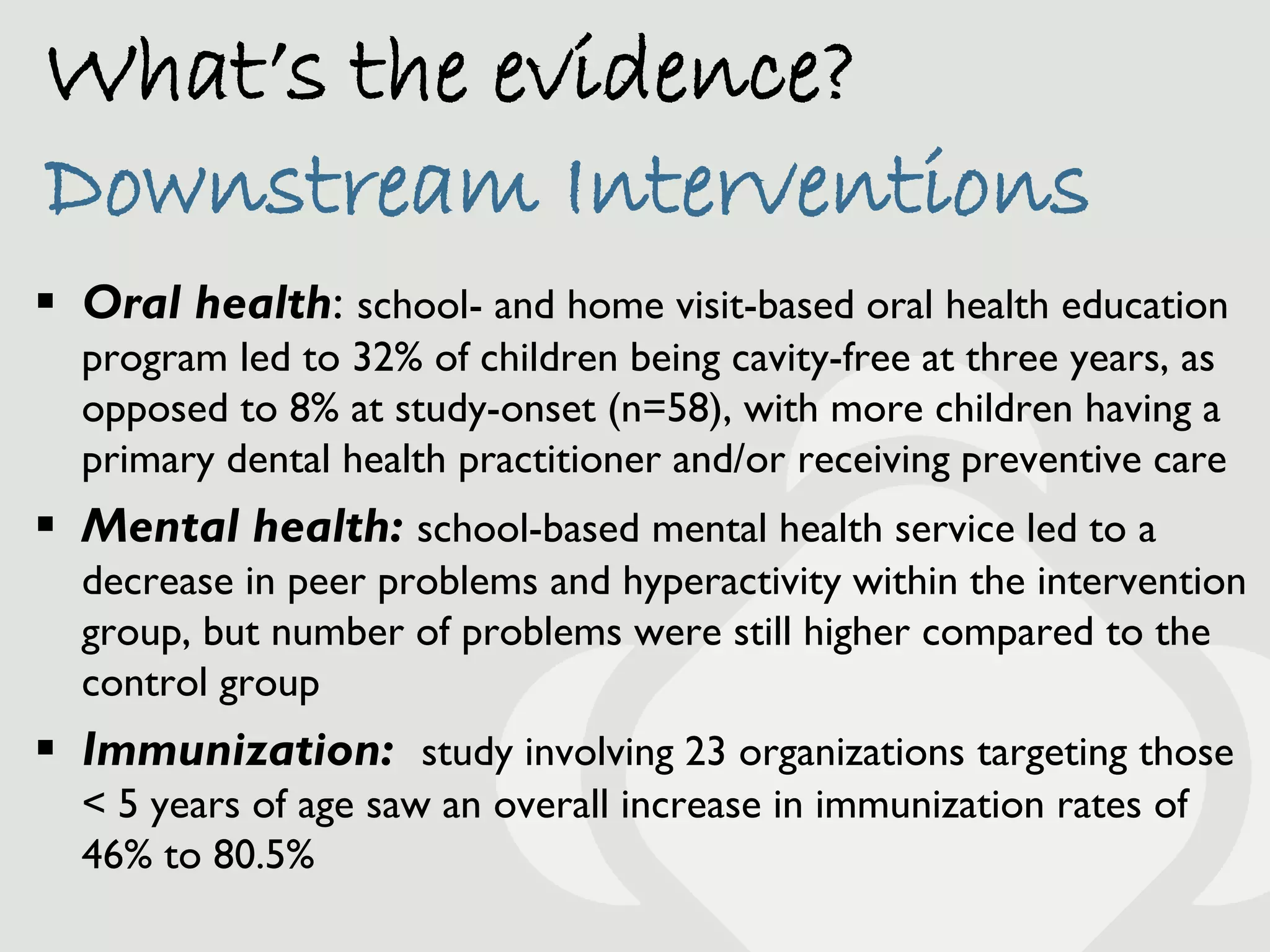
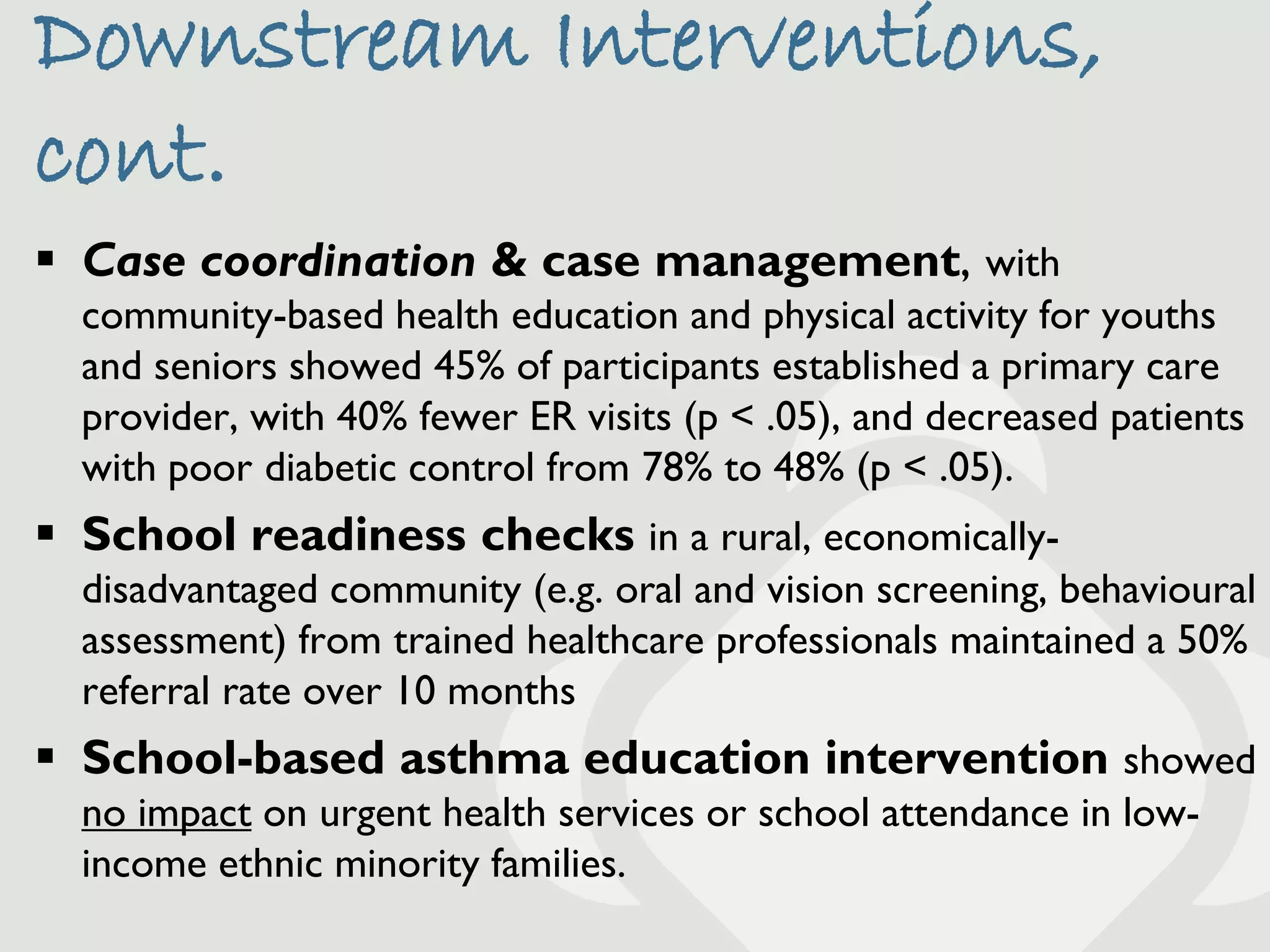
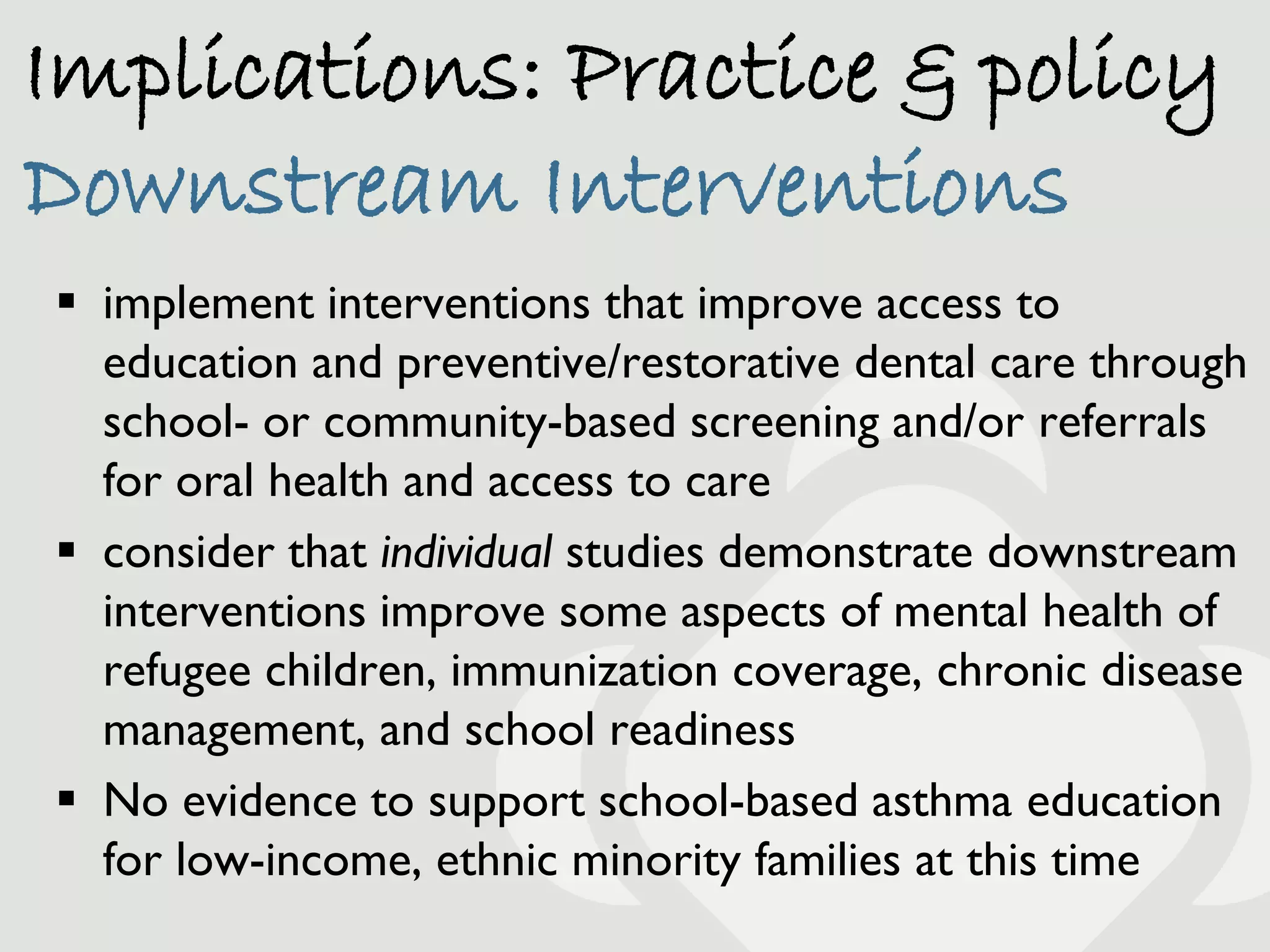
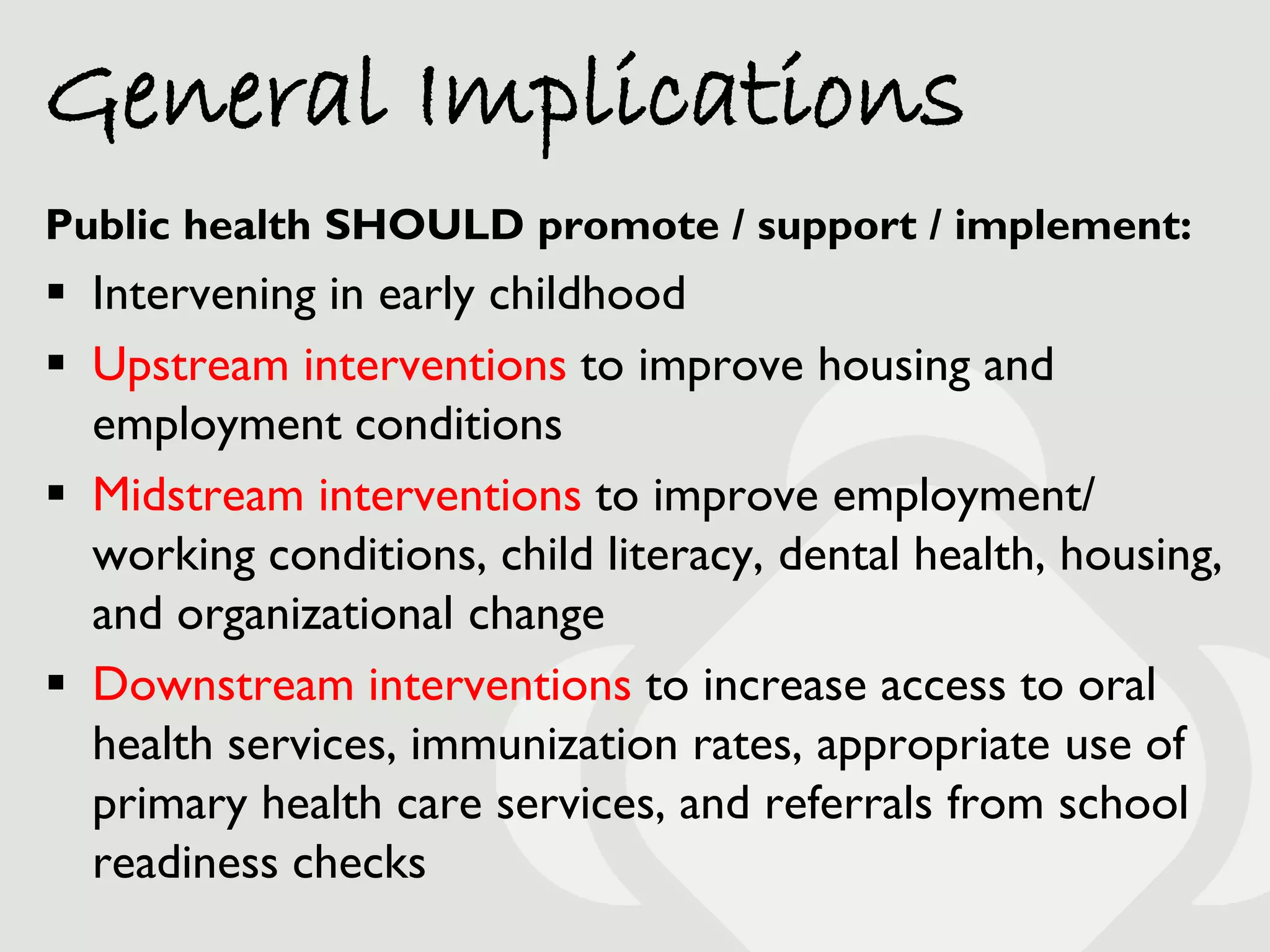


The document outlines a webinar focused on intersectoral action and the social determinants of health (SDH), emphasizing evidence from various studies on effective health interventions. It discusses upstream, midstream, and downstream interventions that aim to improve employment, housing, early childhood literacy, and access to health services, while also noting the limitations and context-specific nature of the findings. Participants are encouraged to engage in evaluations and continue discussions on health equity through designated platforms.































































































