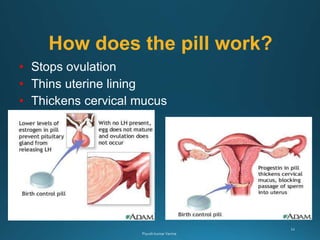
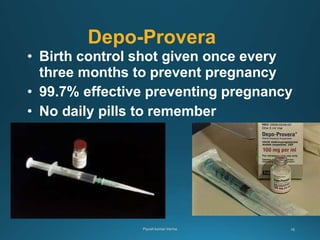
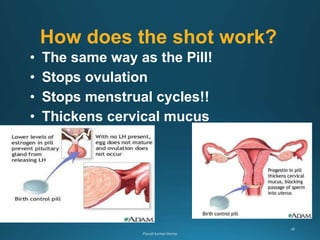
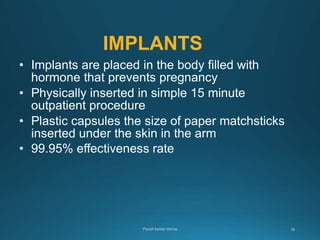
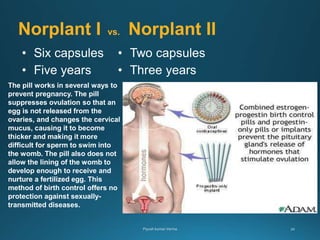
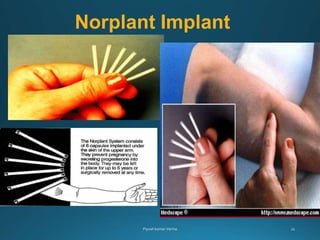
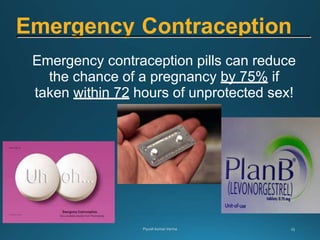
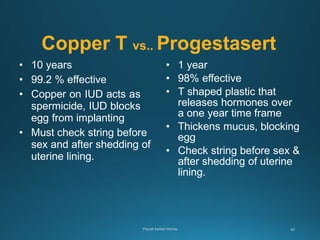
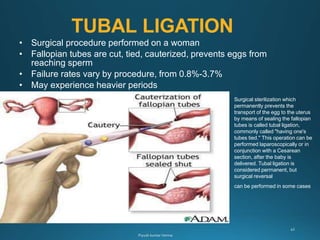
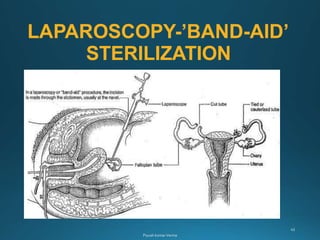
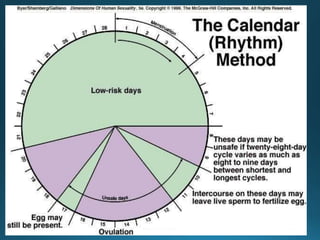
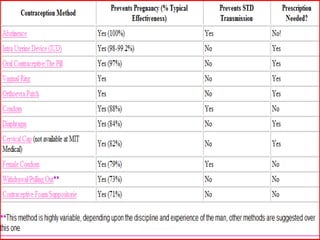
There are several methods of contraception that aim to prevent pregnancy by interfering with ovulation, fertilization, or implantation. Hormonal methods like oral contraceptives and implants work primarily by stopping ovulation. Barrier methods like condoms block sperm from reaching an egg. Long-acting reversible methods like IUDs can prevent fertilization or implantation. Permanent sterilization procedures prevent egg and sperm from meeting. Withdrawal and fertility awareness methods require abstinence from sex during fertile periods. Overall, various contraceptive options exist along a spectrum of effectiveness and reversibility.