
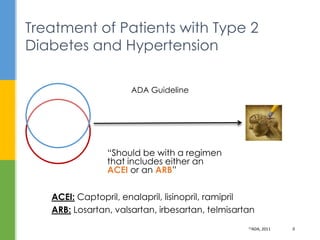
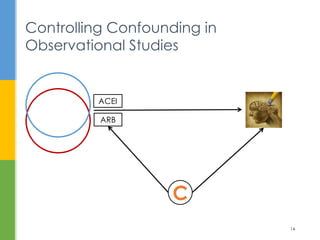
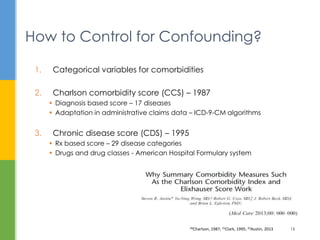
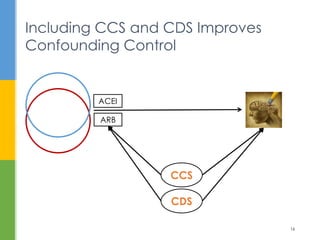
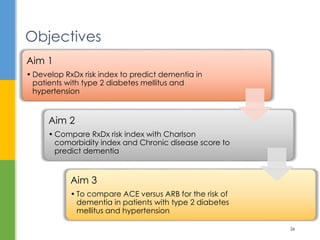

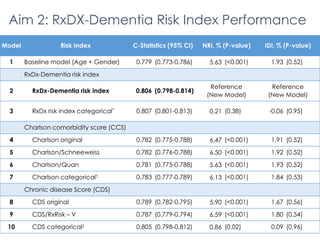
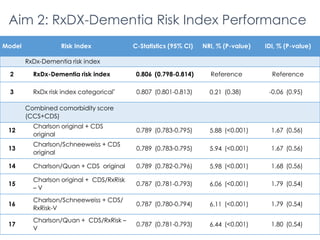
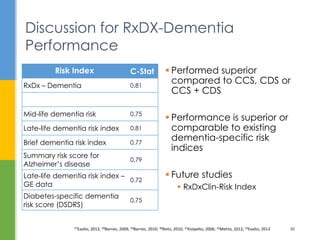
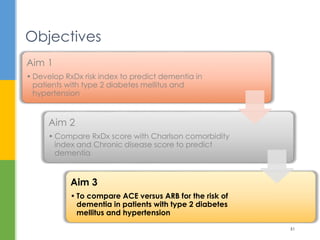
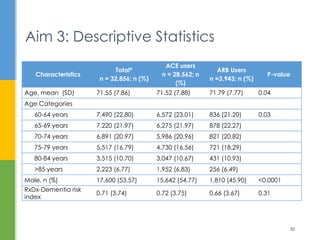
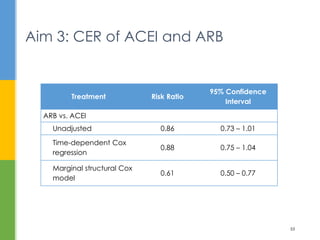




The document examines the comparative effectiveness of ACE inhibitors (ACEI) and angiotensin receptor blockers (ARB) in reducing the risk of dementia in elderly patients with type 2 diabetes and hypertension. It presents a newly developed RXDX risk index aimed at predicting dementia, alongside a comparison of existing comorbidity indices. The study highlights the importance of proper confounding control and provides a methodological framework for future research into dementia risk factors.




























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











