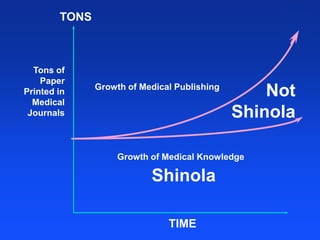
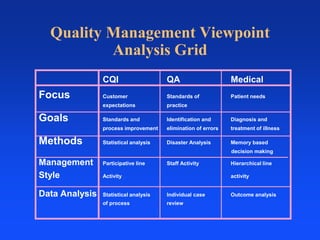
The document discusses the challenges of decision-making in the medical field due to the overwhelming amount of available information and the inefficacy of traditional memory-based systems. It emphasizes the shift towards managed care as a necessary response to cost and quality issues, arguing for the implementation of electronic decision support tools and continuous quality improvement models in healthcare delivery. Additionally, it outlines the principles of total quality management (TQM) and the role of the National Committee for Quality Assurance (NCQA) in enhancing care standards and outcomes.