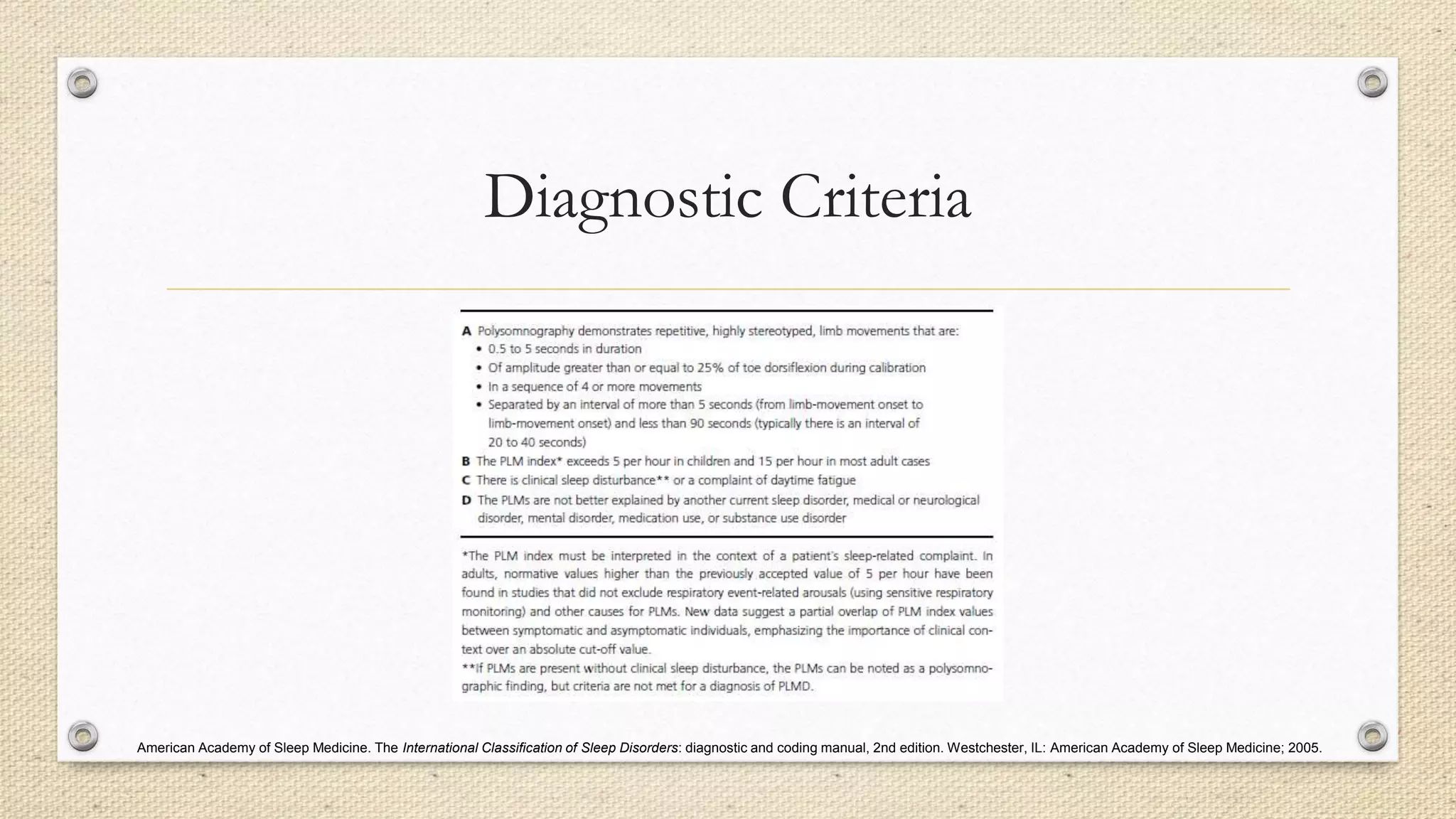
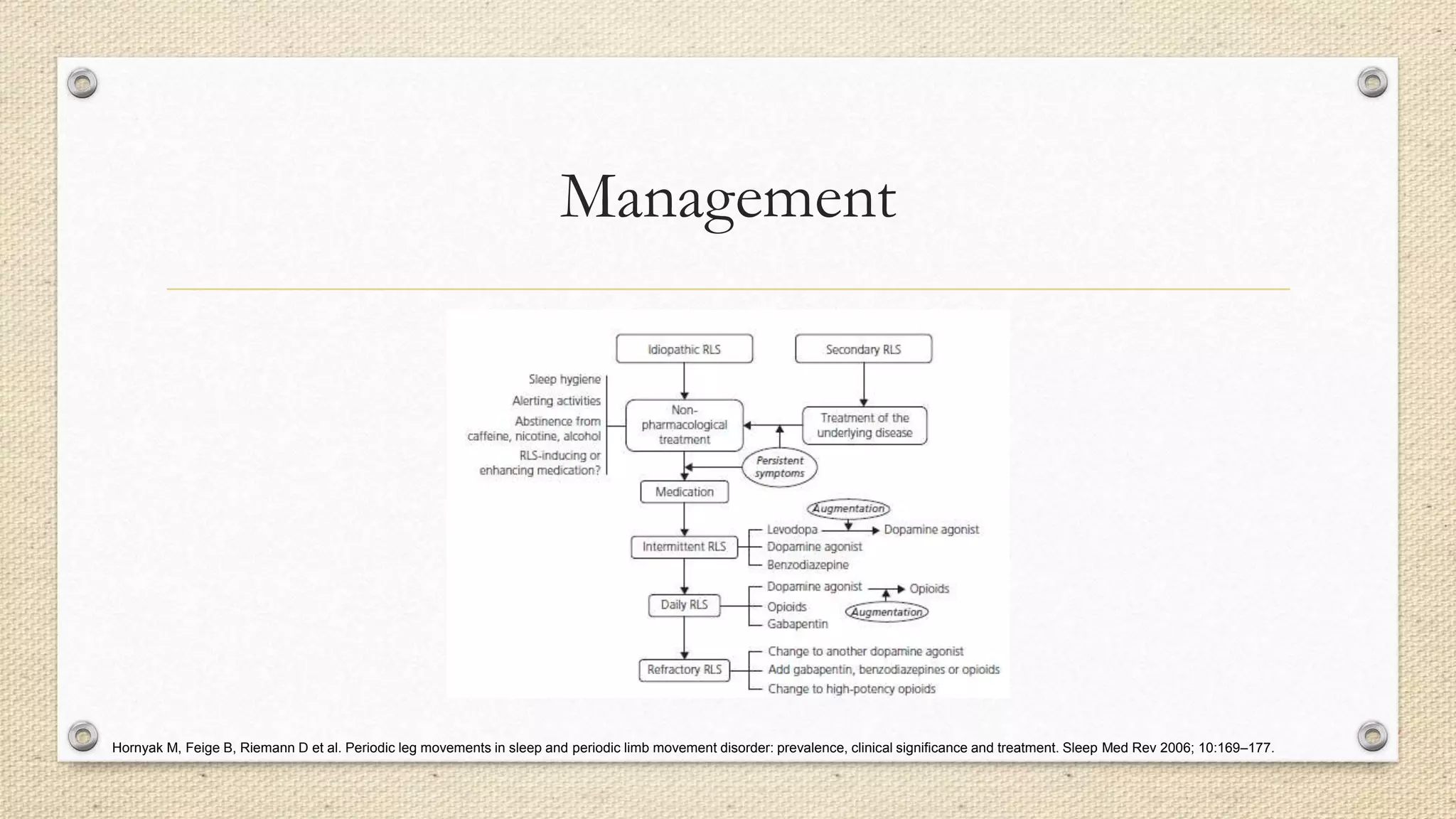
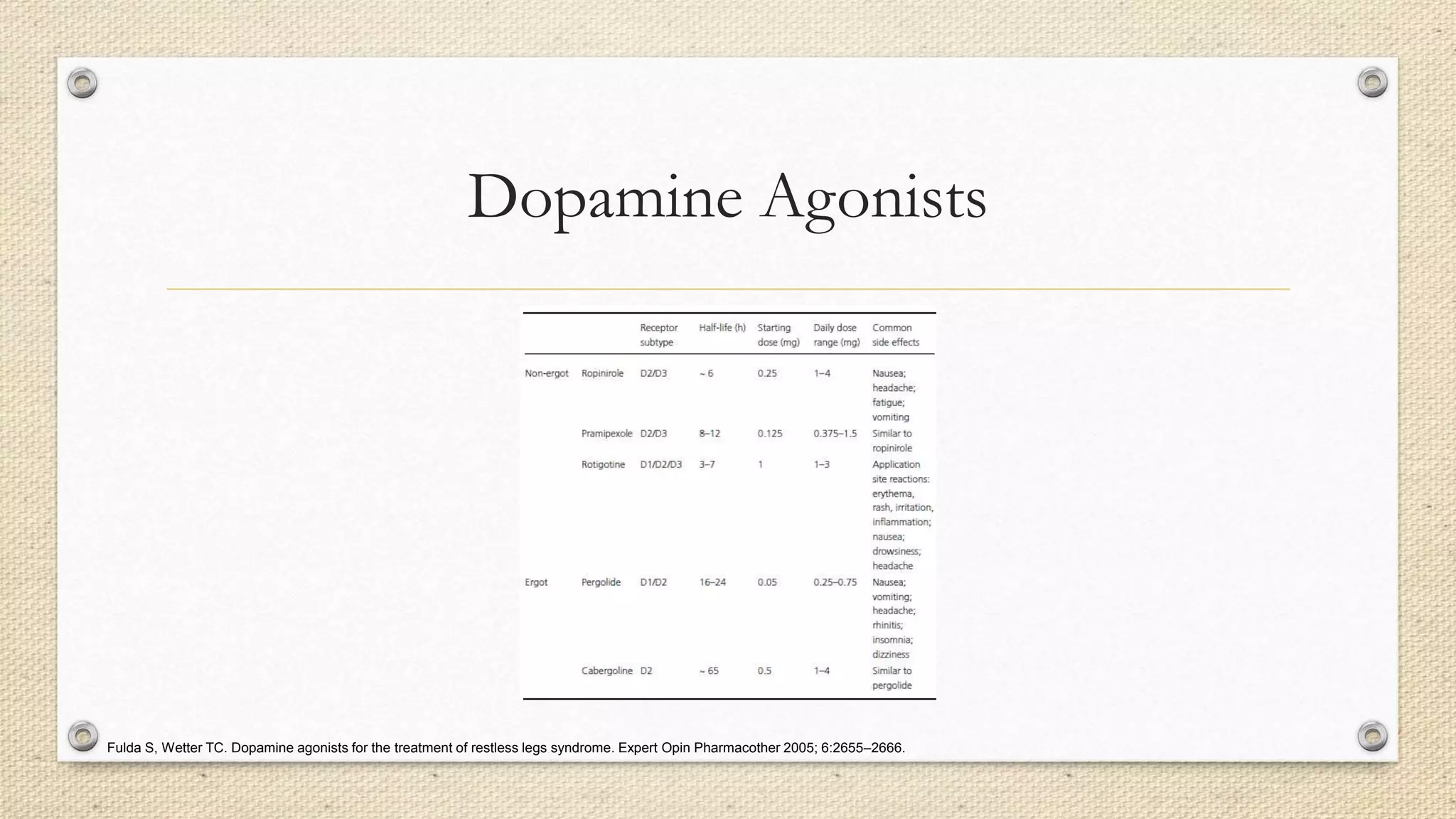
Periodic Limb Movement Disorder (PLMD) is characterized by repetitive, stereotyped leg movements during sleep that resemble a slow version of the peripheral withdrawal reflex. PLMs are commonly seen in patients with Restless Legs Syndrome (RLS) and can negatively impact sleep quality. PLMD is diagnosed when leg movements cause sleep or wakefulness issues and no other sleep disorder is present. Management of PLMD focuses on treating underlying iron deficiency or RLS with iron supplementation, dopamine agonists, opioids, or gabapentin depending on symptoms. Dopamine agonists are first-line but require monitoring for augmentation.