
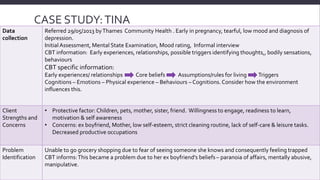
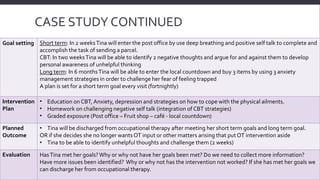
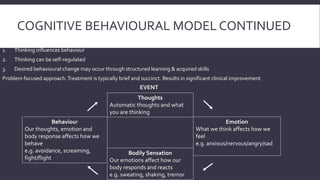

The document outlines a case study on a perinatal mental health client, Tina, who was referred for treatment due to depression and anxiety related to past experiences. It describes her entry criteria, assessment process, cognitive behavioral therapy (CBT) approach, goal setting, and planned interventions aimed at addressing her fears and improving her self-care. The document emphasizes the importance of understanding client's core beliefs and the implementation of gradual exposure to enhance coping strategies and achieve long-term therapeutic goals.