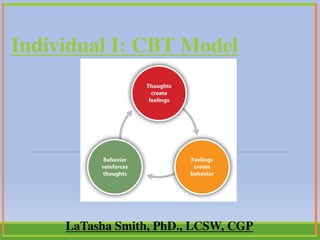
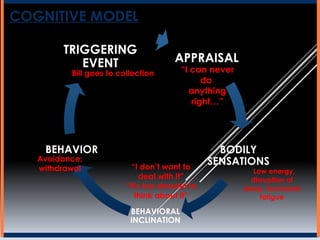
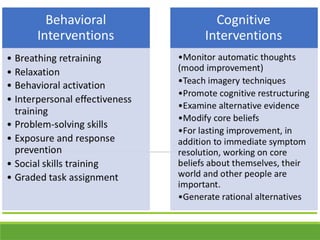
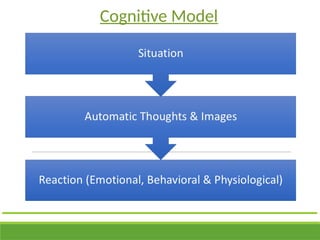
The document outlines the Cognitive Behavioral Therapy (CBT) model, focusing on its principles and goals, particularly the relationship between thoughts, emotions, and behaviors. It discusses the cognitive model and automatic thoughts, emphasizing that recognizing and modifying dysfunctional thinking can lead to emotional and behavioral improvements. It also includes practical exercises for identifying and evaluating automatic thoughts to aid in symptom alleviation.













![Anxiety disorders unit intervention[2]](https://cdn.slidesharecdn.com/ss_thumbnails/anxietydisordersunitintervention2-111028091300-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



































