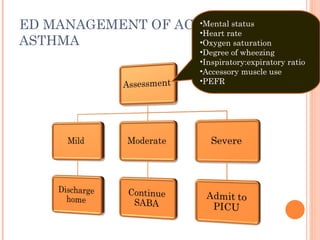
ED MANAGEMENT OFACUTE ASTHMA Mental status Heart rate Oxygen saturation Degree of wheezing Inspiratory:expiratory ratio Accessory muscle use PEFR
17.
ED MANAGEMENT OFACUTE ASTHMA SABA by NEB or MDI-S Up to 3 SABA doses in 1 st hour Oral corticosteroids if incomplete response or if already taking at home
18.
ED MANAGEMENT OFACUTE ASTHMA D/C SABA q 4 hrs for 3-4 days Continue corticosteriod 3-10 days,if begun in ED Continue controller medications Initiate ICS if persistent asthma
19.
ED MANAGEMENT OFACUTE ASTHMA SABA and IB by NEB in 1 st hour Oral corticosteroids If emesis, consider parenteral corticosteriods
20.
ED MANAGEMENT OFACUTE ASTHMA Continue SABA q 30-45 mins or continuously Observe for 60-90 mins after SABA end If sustained response: D/C If minimal or no improvement : admit
21.
ED MANAGEMENT OFACUTE ASTHMA Continue SABA & IB by NEB —consider heliox Consider SQ or IM epinephrine or terbutaline IV corticosteroids Magnesium sulfate IV SABA infusion
22.
ED MANAGEMENT OFACUTE ASTHMA Admit to PICU : Continued severe respiratory distress Altered mental status Need for IV SABA Need for mechanical ventilation Admit others to hospital ward
23.
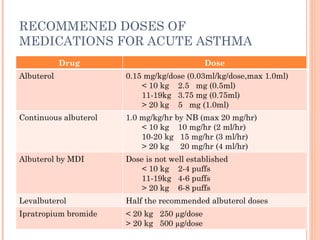
RECOMMENED DOSES OFMEDICATIONS FOR ACUTE ASTHMA Drug Dose Albuterol 0.15 mg/kg/dose (0.03ml/kg/dose,max 1.0ml) < 10 kg 2.5 mg (0.5ml) 11-19kg 3.75 mg (0.75ml) > 20 kg 5 mg (1.0ml) Continuous albuterol 1.0 mg/kg/hr by NB (max 20 mg/hr) < 10 kg 10 mg/hr (2 ml/hr) 10-20 kg 15 mg/hr (3 ml/hr) > 20 kg 20 mg/hr (4 ml/hr) Albuterol by MDI Dose is not well established < 10 kg 2-4 puffs 11-19kg 4-6 puffs > 20 kg 6-8 puffs Levalbuterol Half the recommended albuterol doses Ipratropium bromide < 20 kg 250 µg/dose > 20 kg 500 µg/dose
24.
RECOMMENED DOSES OFMEDICATIONS FOR ACUTE ASTHMA(CONT.) Drug Dose L-epinephrine (1:1000) or terbutaline (1.0 mg/mg) 0.01ml/kg/dose SC or IM (max 0.4 ml) May be repeated every 10-15 min IV terbutaline 10 µg/kg bolus over 10 min,then 0.1-0.3 µg/kg/min infusion Every 30 min,may increase infusion by 0.3 µg/kg/min to a max of 5 µg/kg/min Prednisolone 2 mg/kg (max 60mg), in ED 1 mg/kg/dose bid, home therapy Dexamethasone 0.6mg/kg PO, 2 dose 24 hrs apart IV methylprednisolone 1-2 mg/kg (max 125 mg) IV magnesium sulfate 50-75 mg/kg over 20 min(max 2.5g)
25.
MILD SABA ifnot improve then q 20 mins in 1 st hours Mouthpiecess preferable for older child Decrease nasal filtering of drug Spacer must take 5-8 breaths to complete empty spacer If 3 dose reevaluate
26.
SHORT ACTING BETA2-AGONISTSIN ACUTE ASTHMA IB= ipratropium bromide MDI-s=metered dose inhaler with spacer NHLBI=national,Heart,Lung and blood institute Mild Moderate Severe Delivery method Intermittent NEB or MDI-S Continuous by NEB for 1 hr, then reassess Consider SC or IM Continuous by NEB Comments Most patients will need 1-2 treatments Allow for MDI-S teaching No IB needed Not superior to MDI-S Easier to adhere to NHLBI guidelines for the first hr of therapy Concurrent IB therapy is more easily delivered Better outcomes in severe asthma
BRONCHIOLITIS Seasonal disease: November &April Nearly all children : affected virus cause bronchiolitis at least once during first 2 years of life More common < 1 year
29.
Increased mucus secretion,cell death, and sloughing, a peribronchiolar lymphocytic infiltrate and submucosal edema Combination of debris&edema produces critical narrowing & obstruction of small airways .
30.
BRONCHIOLITIS M/C CAUSE: RESPIRATORY SYNCYTIAL VIRUS (RSV) Age < 3 mo Preterm GA < 34 wks Toxic or ill general appearance RR > 70/min SpO2 <95% CXR : atelectasis Breast feeding < 1 mo Maternal smoking RSV subtype A Male Air pollution environment Severity associate with
31.
SUGGEST BRONCHIOLITIS ASSESSMENTTOOL Mild Moderate Severe Feeding Normal Less Poor SaO2 in room air ≥ 95 % 92 -94 % < 92 % Respiratory rate(/min) < 60 60 - 70 > 70 Retraction None/ minimal Intercostal Substernal Accessory muscle use None None Neck or abdominal Wheeze None/minimal Moderate expiratory Severe inspiratory/expiratory, audible without stethoscope Air exchange Good, equal breath sound Localized decrease breath sound Multiple area of decrease breath sound
32.
ED MANAGEMENT OFBRONCHIOLITIS Improved Not Improved Improved Not Improved
33.
PROPHYLAXIS ED :No role preventive medication in ED Education Advice Palivizumab (Synagis) Monoclonal antibodies againt RSV Specific immune globulin Not effect acute process Effective in reducing hospitalization in high risk group (monthly IM during high prevalence month ) Recommended for most age < 24 month with Chronic lung disease Congenital heart disease Prematurity
HTTP://EMEDICINE.MEDSCAPE.COM/ARTICLE/800428-TREATMENT PEDIATRIC BRONCHIOLITIS: DIFFERENTIAL DIAGNOSES & WORKUP AUTHOR: MARK LOUDEN, MD, FACEP, ASSISTANT MEDICAL DIRECTOR, EMERGENCY DEPARTMENT, DUKE RALEIGH HOSPITAL CONTRIBUTOR INFORMATION AND DISCLOSURES UPDATED: DEC 27, 2010
42.
43.
44.
http://emedicine.medscape.com/article/800428-treatment Pediatric Bronchiolitis: Differential Diagnoses & Workup Author: Mark Louden, MD, FACEP, Assistant Medical Director, Emergency Department, Duke Raleigh Hospital Contributor Information and Disclosures Updated: Dec 27, 2010
#30 Infection of bronchiolar respiratory and ciliated epithelial cells produces increased mucus secretion, cell death, and sloughing, followed by a peribronchiolar lymphocytic infiltrate and submucosal edema. The combination of debris and edema produces critical narrowing and obstruction of small airways.










































![Croup / โรคหลอดลมอักเสบ ฮอร์โมนอะดรีนาลีน Racemic รักษาโรคซาง [14] [ 15] Racemic อะดรีนาลีนเป็นส่วนผสมของ dextrorotatory (D) 1:1 และ levorotatory (L) isomers ของอะดรีนาลีน [16] l แบบเป็นส่วนประกอบที่ใช้งานอยู่ [16] Racemic อะดรีนาลีนทำงานโดยการส่งเสริมของผู้รับในเส้นทางการบินกับผลลัพธ์ mucosal α - adrenergic vasoconstriction และลดอาการบวมน้ำ และสิ่งเร้าที่ β - adrenergic subglottic ผู้รับผลแห่งการผ่อนคลายกล้ามเนื้อเรียบหลอดลม [15]](https://image.slidesharecdn.com/pedrespiemergencylower-110315131206-phpapp01/85/Pediatric-respiratory-emergency-lower-45-320.jpg)

















































