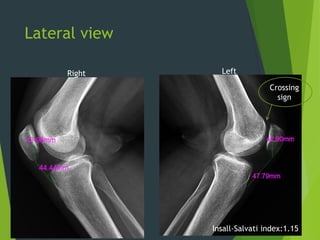
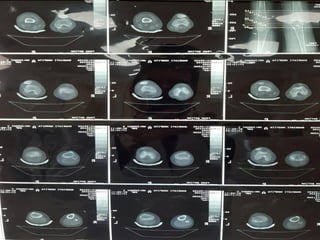
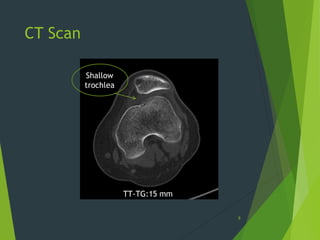
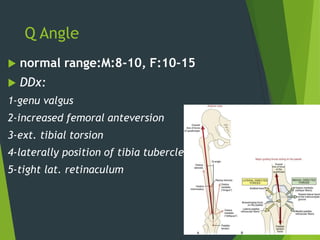
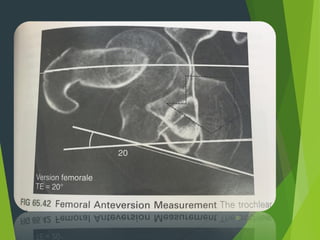
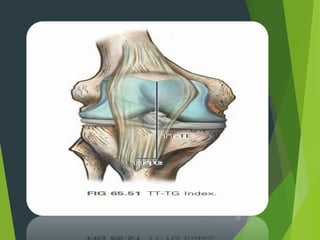
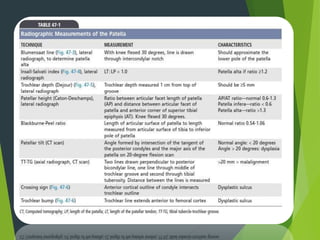
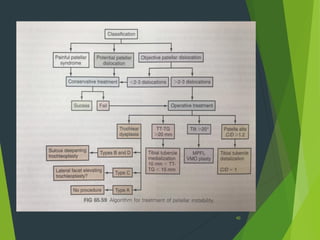
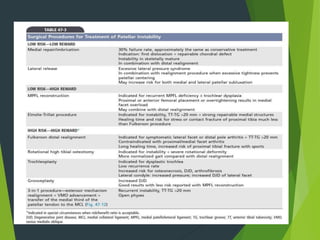
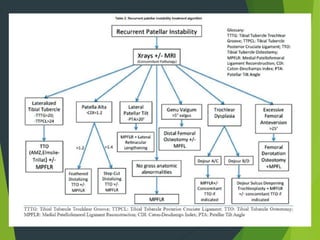
This document presents two case studies of patellofemoral instability. Case one involves a 40-year-old female with a history of patellar dislocation and recurrent instability. Physical exam reveals positive tests for instability. Radiographs show a crossing sign and Insall-Salvati index of 1.15. Case two is a 33-year-old female with a history of patellar instability and failed non-operative treatment. Radiographs show femoral anteversion of 24 degrees and increased TT-TG distances. The document discusses anatomy, biomechanics, symptoms, exam findings, imaging, and surgical and non-surgical treatment options for patellofemoral instability.





























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






