Download as PDF, PPTX








![-“các bẫy bạch cầu trung tính ngoại bào” (“neutrophil extracellular
traps” – NETS)
-trophoblasts : nguyên bào nuôi
-decidual cells : tb thuộc màng rụng
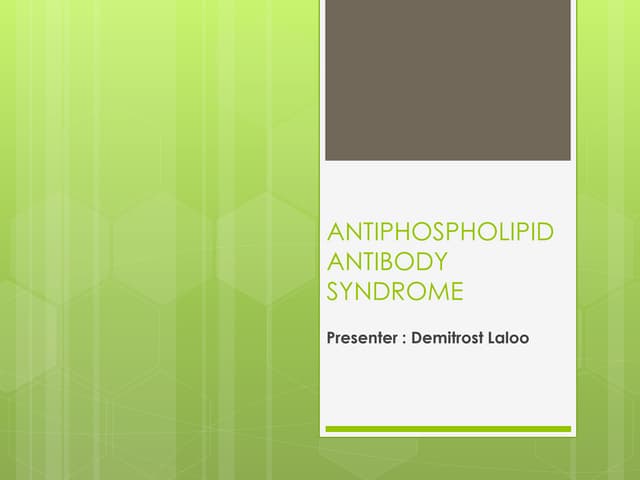
Figure 1. Summary of the Proposed Pathogenesis of Antiphospholipid-Antibody–Mediated Clinical
Problems.
In Panel A, antiphospholipid antibodies are produced by B cells; binding to anionic surfaces
converts the closed, nonimmunogenic β2-glycoprotein I (β2GPI) to the open, immunogenic β2GPI.
In Panel B (left), antiphospholipid antibodies bind to the immunogenic β2GPI, resulting in
endothelial-cell, complement, platelet, neutrophil, and monocyte activation (including the release
of neutrophil extracellular traps [NETosis]).
In Panel B (middle), antiphospholipid antibodies promote clot formation, and in Panel B (right),
antiphospholipid antibodies interfere with trophoblasts and decidual cells.
Panels C and D show that, on the basis of multiple mechanisms that are not mutually exclusive,
antiphospholipid antibodies result in inflammation, vasculopathy, thrombosis, and pregnancy
complications.](https://image.slidesharecdn.com/pas-230209101018-f56059c6/85/PAS-LN-1-pdf-9-320.jpg)












































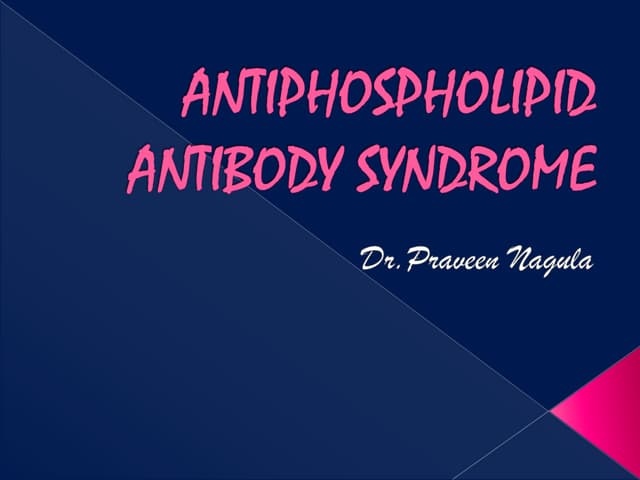
![A proposed treatment protocol for the induction and maintenance management of histologically class III, IV, and V lupus nephritis in
children as based on published recommendations [14,15,16,17,18]. CR, complete response (UPCR < 50 mg/mmol, normal kidney function);
PR, partial response (> 50% reduction in proteinuria, not nephrotic, normal kidney function). UPCR, urine protein:creatinine ratio; LN, lupus
nephritis; DMARD, disease modifying anti-rheumatic drug; CR, complete response; PR, partial response; MMF mycophenolate mofetil;
AZA, azathioprine; IV, intravenous; CNI, calcineurin inhibitor
Pediatric Nephrology (2021) 36:1377–1385](https://image.slidesharecdn.com/pas-230209101018-f56059c6/85/PAS-LN-1-pdf-54-320.jpg)




The document discusses antiphospholipid antibodies in pediatric lupus nephritis. It defines antiphospholipid antibody syndrome as an autoimmune disorder that can manifest as recurrent thrombosis. It also defines systemic lupus erythematosus as an autoimmune disease that can damage organs like the kidneys, skin, blood cells, and nervous system. Antiphospholipid antibodies are found to be associated with clinical symptoms like thrombosis and pregnancy complications in pediatric lupus nephritis patients.