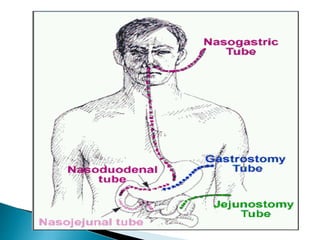
Multiple factors can contribute to malnutrition, including inadequate food intake, increased nutritional demands from illness, impaired digestion or absorption, and metabolic issues. Malnutrition can develop gradually or suddenly and result in impaired immune function, reduced muscle strength, respiratory issues, impaired wound healing, infections, delayed recovery from illness, and reduced quality of life. Parenteral nutrition is used when oral or enteral nutrition is not possible or sufficient and involves the intravenous administration of balanced nutrients including amino acids, glucose, lipids, vitamins, minerals, and electrolytes to meet nutritional needs. Close monitoring is needed to ensure nutritional support meets the patient's requirements.


























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












