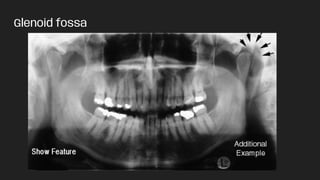
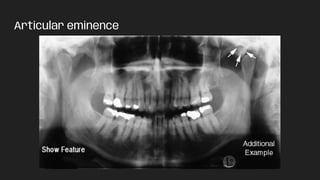
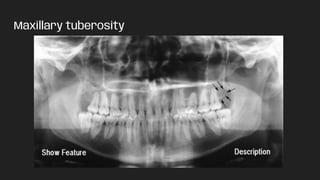
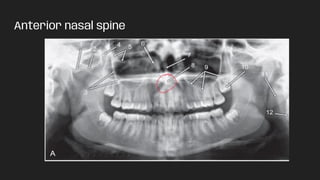
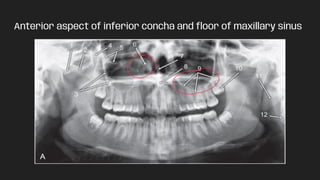
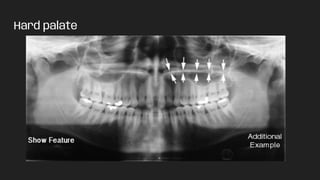
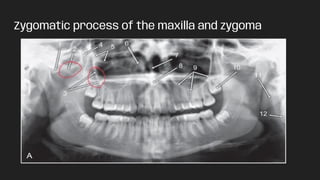
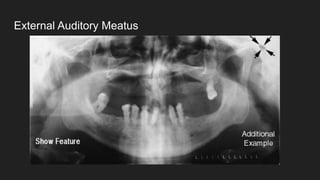
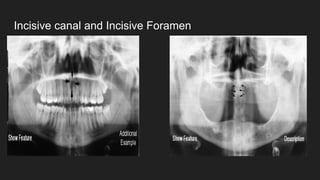
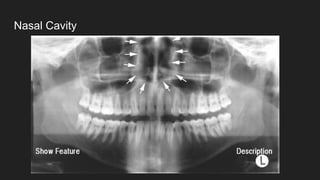
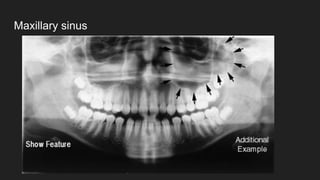
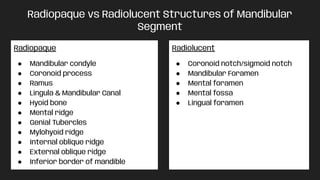
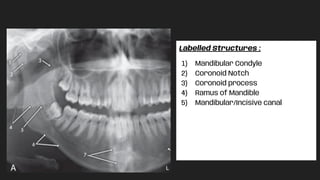
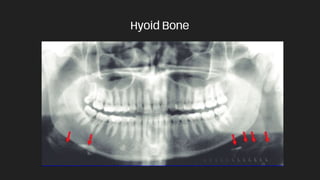
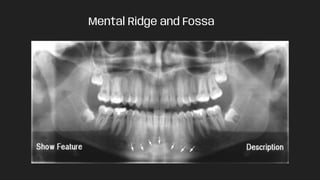
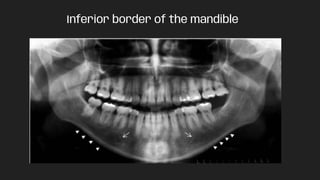
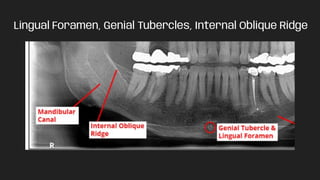
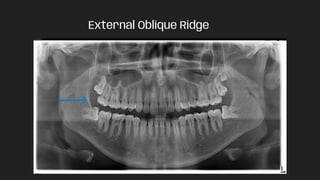
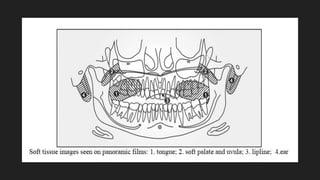
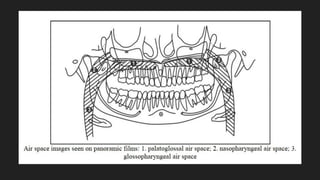
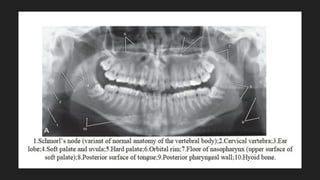
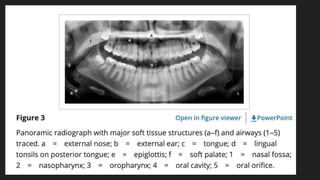
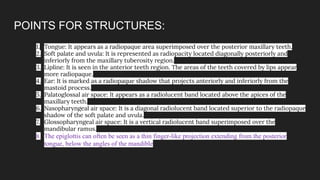
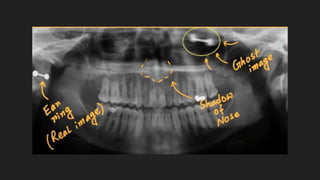
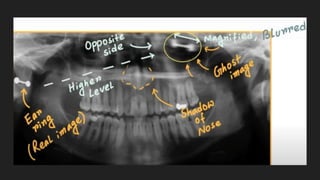
The document discusses the anatomy and structures visualized in panoramic radiographs, focusing on various landmarks in the midfacial region and mandible, including both radiopaque and radiolucent features. It details specific structures such as the mastoid process, glenoid fossa, and various projections of the mandible. Additionally, it explains ghost images as artifacts that occur due to certain objects in the x-ray path.









































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



