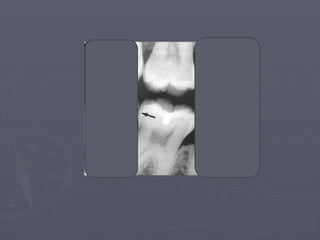
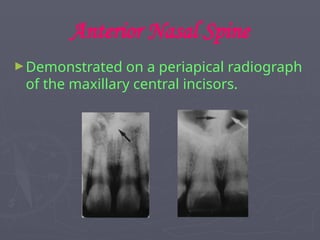
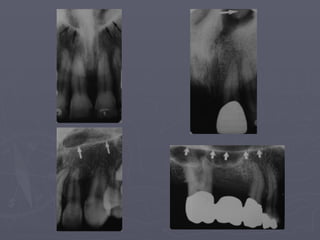
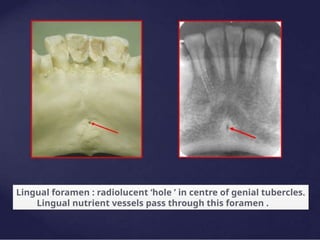
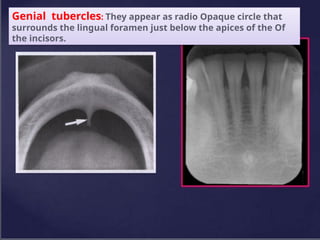
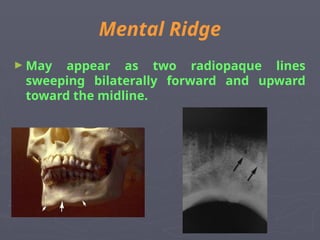
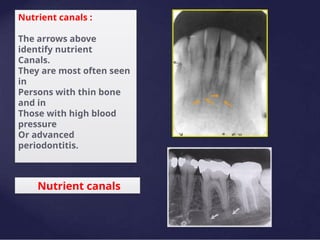
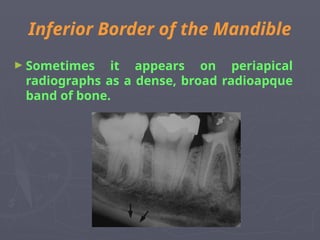
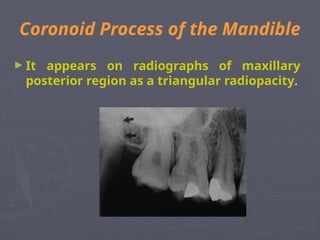
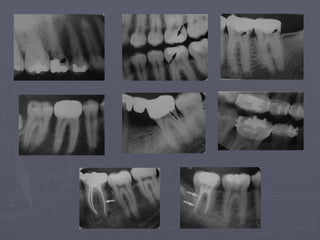
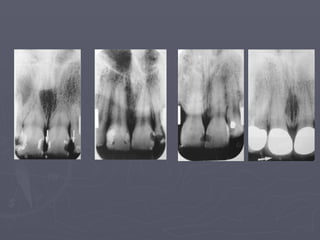
This document discusses the radiographic anatomy essential for recognizing diseases, emphasizing the importance of understanding normal structures and their variations. It details the radiographic appearances of teeth, supporting structures, and the maxilla and mandible, including the identification of various radiopaque and radiolucent landmarks. The document also covers restorative materials and their radiographic characteristics, aiding in the diagnosis and assessment of oral health.

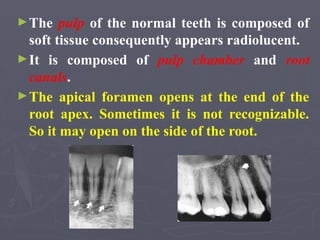














































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















