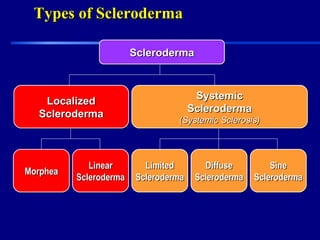
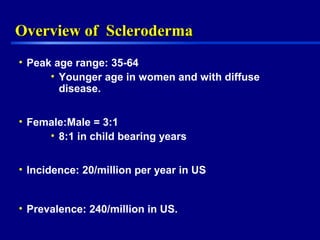
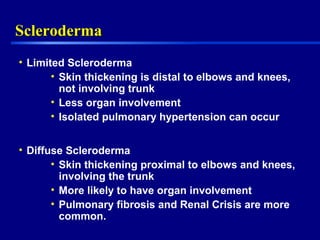
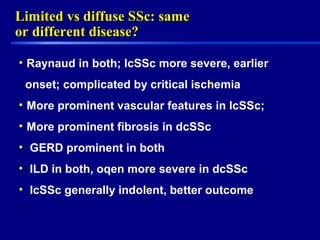
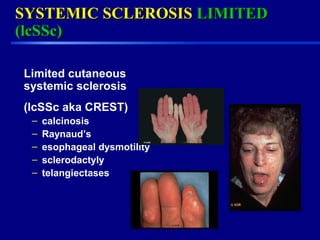
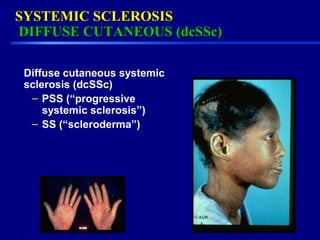
This document provides an overview of scleroderma, a multisystem disorder characterized by skin thickening and organ involvement, with a focus on patient education and support. The Scleroderma Foundation aims to assist patients and research a cure while discussing the classification of scleroderma into limited and diffuse types, as well as the importance of early diagnosis and treatment. Various therapeutic options and challenges in managing the disease are also addressed, highlighting the need for individualized approaches and better treatments.



































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



