




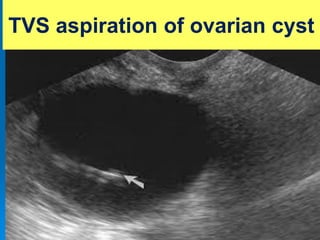
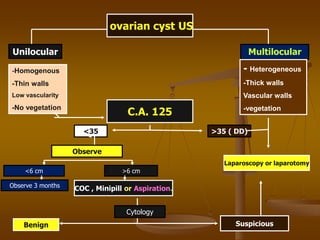
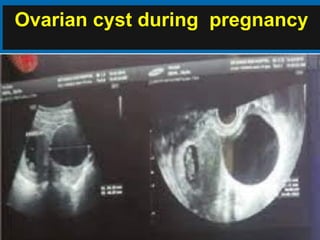
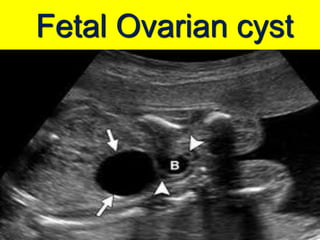
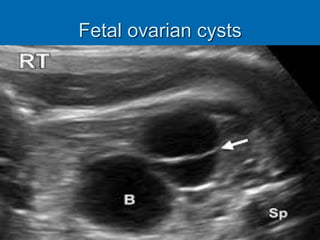

Ultrasonic-guided ovarian cyst aspiration can be performed by gynecologists as an alternative to laparoscopy or laparotomy in certain situations. There are 4 main indications for aspiration: 1) functional cysts, 2) cysts during the second trimester of pregnancy, 3) fetal ovarian cysts, and 4) retention cysts during GnRH analogue treatment. Strict criteria like transvaginal ultrasound findings and CA-125 levels should be followed to exclude malignancy. While aspiration has advantages of less invasiveness and faster recovery, disadvantages include possible recurrence, inconclusive cytology, and potential dissemination of neoplastic cells if present. Close follow-up is important after any aspiration
































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









