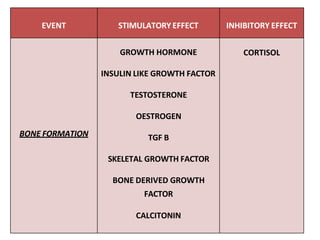
Osteoporosis is a disease characterized by low bone mass and structural deterioration of bone tissue, leading to bone fragility and an increased risk of fractures. Key points:
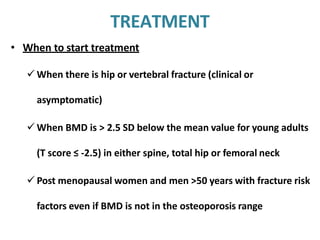
- It is defined as a bone density 2.5 standard deviations or more below the mean bone density of healthy young adults.
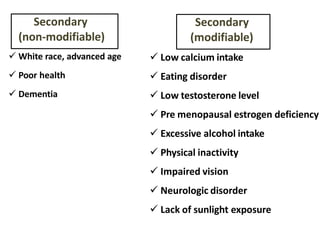
- It occurs more frequently with age and is more common in women, especially after menopause due to estrogen loss.
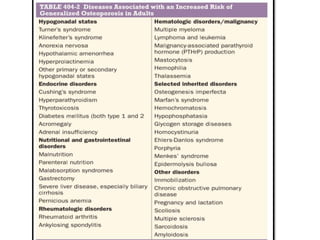
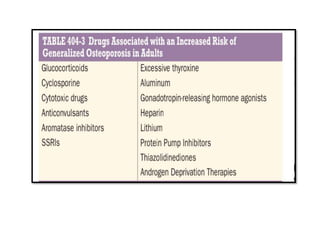
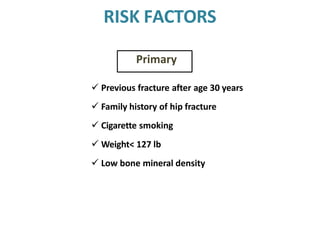
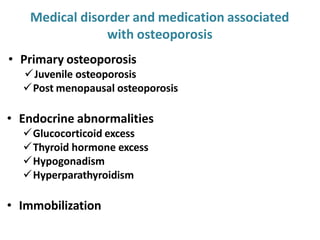
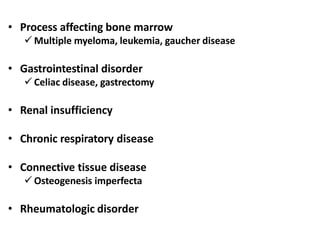
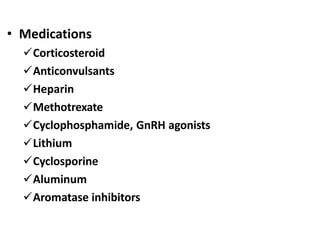
- Risk factors include family history, smoking, low weight, inactivity, excessive alcohol, and certain medical conditions or medications.
- It is usually asymptomatic until a fracture occurs. Treatment focuses on lifestyle changes, calcium/vitamin D supplementation, and medications to increase bone density


























































![Chapter_01_Anatomy_of_Skin[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/chapter01anatomyofskin1-230409112654-4252e8d1-thumbnail.jpg?width=640&height=640&fit=bounds)