This document provides an overview of osteoporosis including its definition, characteristic features, classification, contributing factors, clinical manifestations, investigations, diagnosis, and treatment. Some key points:
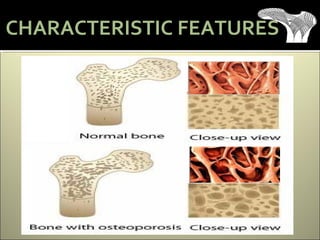
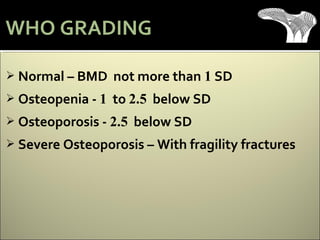
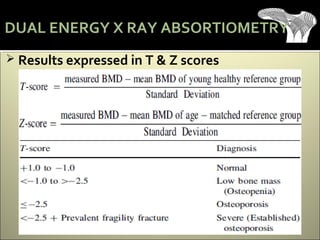
- Osteoporosis is a skeletal disorder characterized by low bone mass and deterioration of bone tissue, resulting in fragile bones and increased fracture risk. It is defined by the WHO as a bone density 2.5 standard deviations below the mean for young healthy adults.
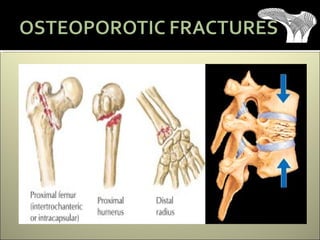
- It is asymptomatic until a fracture occurs. Common fractures are of the distal radius, vertebral bodies, and hip. Risk factors include age, sex, family history, smoking, alcohol, low body weight, and estrogen deficiency.
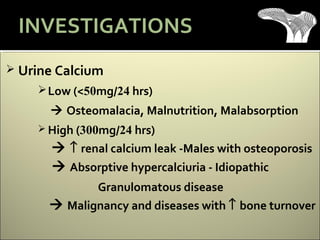
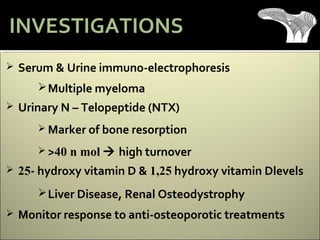
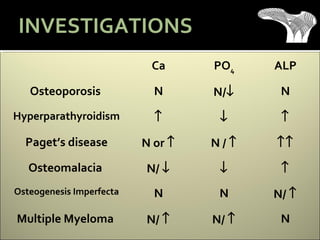
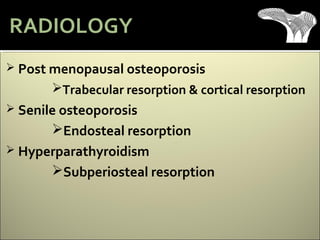
- Diagnosis involves investigations






























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








