


























![International Menopause Society Recommendations –
2016
An appropriate assessment of prevalent fractures and secondary causes of
osteoporosis should precede any therapeutic decisions
Lifestyle strategies should be part of any treatment strategy [A]
Choice of pharmacological therapy should be based on a balance of
effectiveness, risk and cost
MHT is the most appropriate therapy for fracture prevention in early
menopause](https://image.slidesharecdn.com/osteoporosismenopause-220615072253-e5cfe379/75/Osteoporosis-Menopause-pptx-30-2048.jpg)













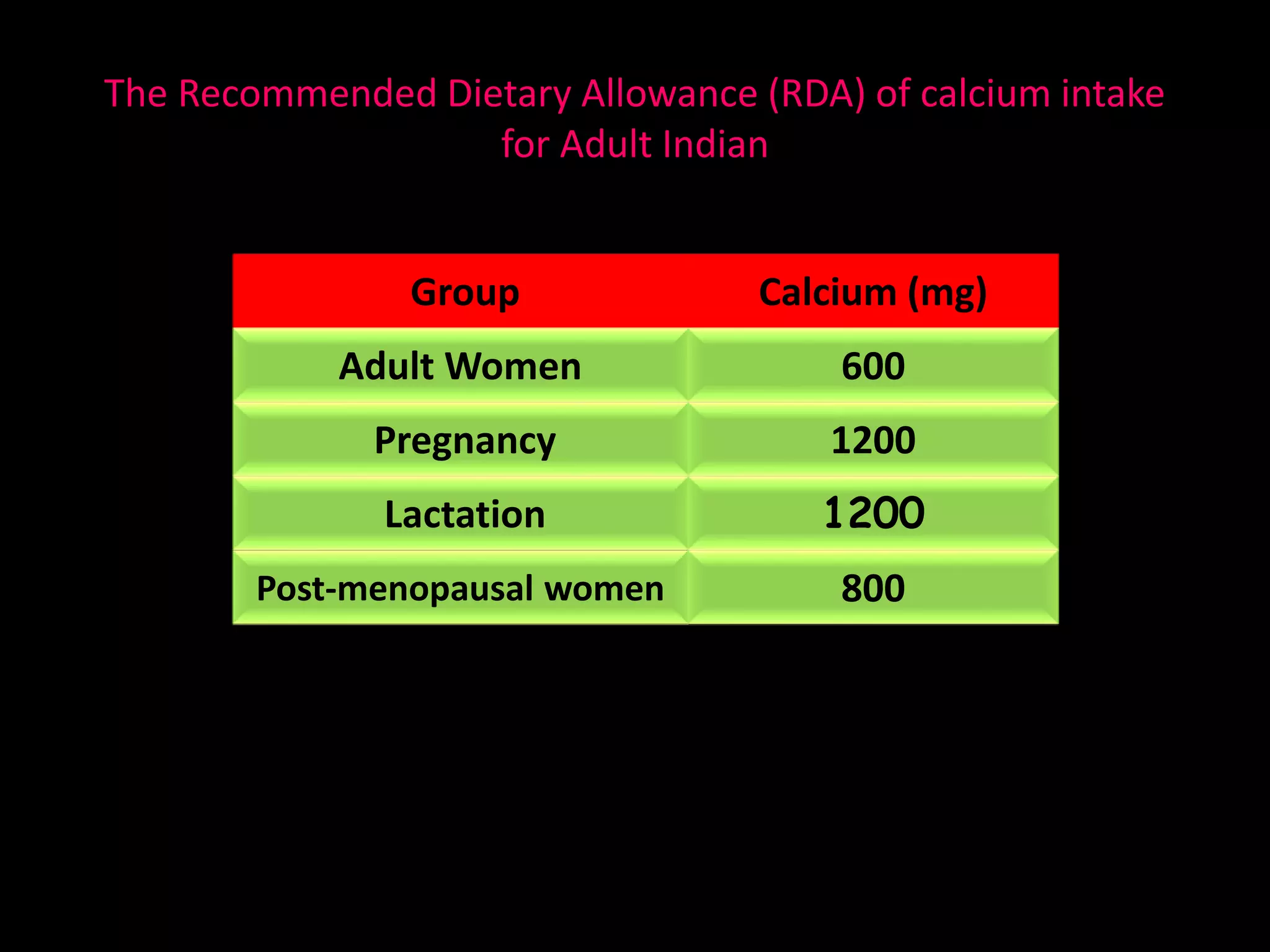
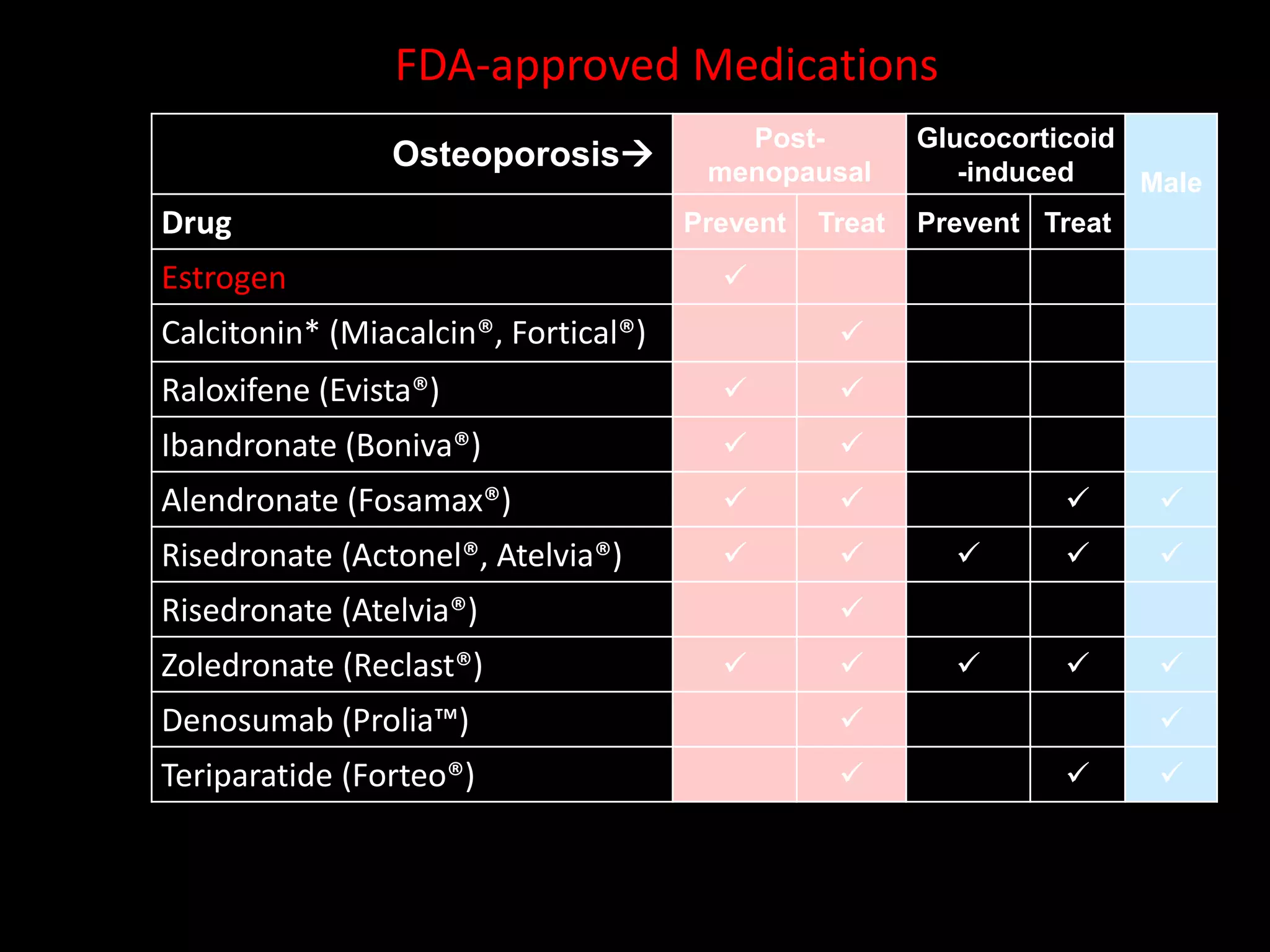
This document discusses osteoporosis and menopause. It defines osteoporosis as a skeletal disorder characterized by compromised bone strength, which increases the risk of fractures. Key risk factors for osteoporosis include being postmenopausal, having a family history, lack of exercise, low calcium intake, vitamin D deficiency, smoking, and certain medical conditions or medications. The document reviews guidelines for testing and treating osteoporosis, including using bone mineral density (BMD) tests and the FRAX score to determine treatment. Lifestyle changes like exercise, calcium/vitamin D intake, and avoiding smoking are recommended to improve bone health. The document also discusses medications used to treat osteoporosis such as








































![Osteoporosis%203rd%20yr[1]](https://cdn.slidesharecdn.com/ss_thumbnails/osteoporosis203rd20yr1-111103005118-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)














































