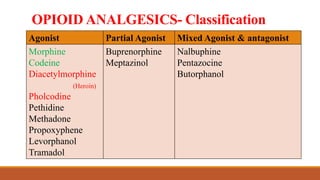
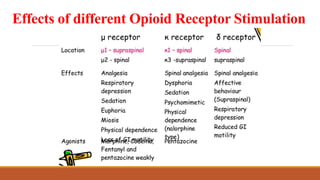
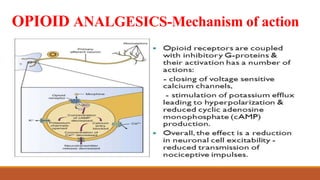
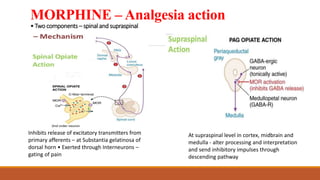
Opioid analgesics are drugs that selectively relieve pain by acting in the central nervous system or on peripheral pain mechanisms without significantly altering consciousness. There are several classifications of opioids including agonists, partial agonists, mixed agonists/antagonists. Morphine is an agonist that provides strong analgesia through inhibition of excitatory neurotransmitters in the spinal cord and altering pain processing in the brain. Adverse effects include respiratory depression, vomiting, sedation, and dependence/tolerance with repeated use. Opioids are commonly used to treat severe pain from fractures, myocardial infarction, cancer, burns and post-operatively.