Downloaded 682 times
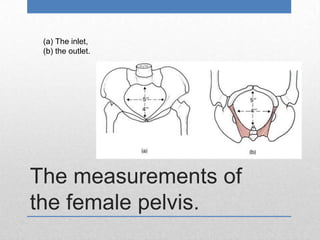
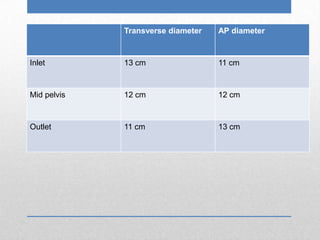
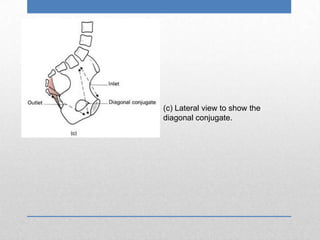

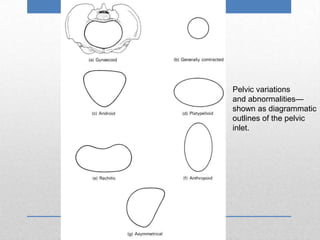

The document describes measurements of the female pelvis, including the transverse and anteroposterior diameters of the inlet, mid-pelvis, and outlet. It notes that the most useful clinical measurement is the diagonal conjugate from the pubic symphysis to the sacrum. Variations in pelvic shape include the gynaecoid, android, platypelloid, and anthropoid types. Common abnormalities that affect the pelvic inlet include symmetrical contraction, rickets-induced flattening, and asymmetry from various causes.