1) Diabetes is a group of metabolic disorders characterized by high blood sugar levels. It includes defects in insulin secretion, insulin action, or both.
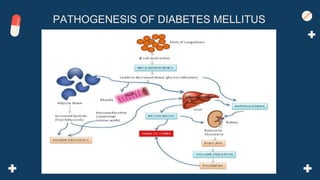
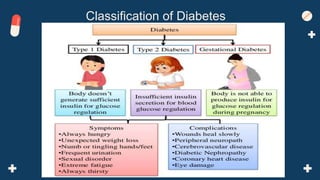
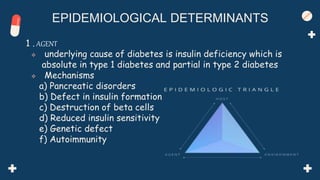
2) The document discusses the classification, pathogenesis, epidemiology, diagnostic criteria and methods, and control and prevention of diabetes globally and in India.
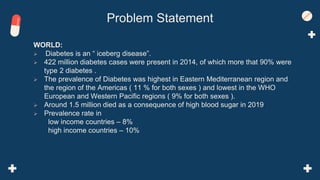
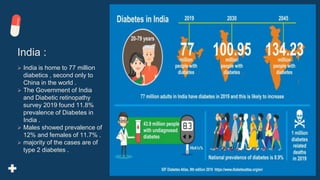
3) It provides statistics on the prevalence of diabetes worldwide and in India, making it one of the most common non-communicable diseases. Prevention and control involves lifestyle changes, medication and national programmes.

























































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)














