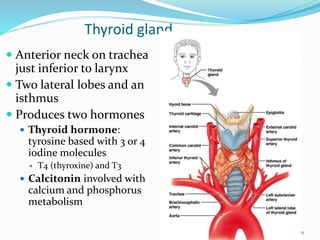
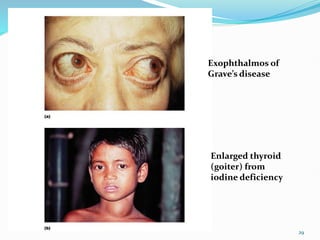
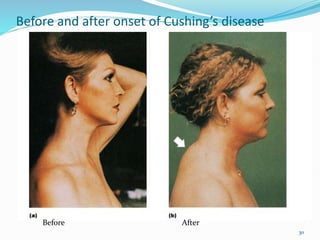
The document discusses several endocrine disorders and conditions involving hormone imbalances. It covers disorders of the pituitary gland like gigantism and acromegaly caused by excess growth hormone, as well as diabetes insipidus caused by excess antidiuretic hormone. Disorders of the thyroid like Graves' disease, and of the adrenal glands like Cushing's syndrome and Addison's disease are also outlined. The effects and roles of various hormones produced by these and other endocrine glands like the pancreas and gonads are described.




















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















