
Recommended
Recommended
More Related Content
Similar to November-December 2013 • Vol. 22No. 6 359Beverly Waller D.docx
Similar to November-December 2013 • Vol. 22No. 6 359Beverly Waller D.docx (20)
More from picklesvalery
More from picklesvalery (20)
Recently uploaded
Recently uploaded (20)
November-December 2013 • Vol. 22No. 6 359Beverly Waller D.docx
- 1. November-December 2013 • Vol. 22/No. 6 359 Beverly Waller Dabney, PhD, RN, is Associate Professor, Southwestern Adventist University, Keene, TX. Huey-Ming Tzeng, PhD, RN, FAAN, is Professor of Nursing and Associate Dean for Academic Programs, College of Nursing, Washington State University, Spokane, WA. Service Quality and Patient-Centered Care L eaders of the U.S. Depart - ment of Health & Human Services (2011) urge providers to improve the overall quality of health care by making it more patient centered. Patient-centered care (or person-centered care) refers to the therapeutic relationship between health care providers and recipients of health care services, with emphasis on meeting the needs of individual patients. Al - though the term has been used widely in recent years, it remains a poorly defined and conceptualized phenomenon (Hobbs, 2009).
- 2. Patient-centered care is believed to be holistic nursing care. It pro- vides a mechanism for nurses to engage patients as active partici- pants in every aspect of their health (Scott, 2010). Patient shadowing and care flow mapping were used to create a sense of empathy and urgency among clinicians by clarify- ing the patient and family experi- ence. These two approaches, which were meant to promote patient-cen- tered care, can improve patient sat- isfaction scores without increasing costs (DiGioia, Lorenz, Greenhouse, Bertoty, & Rocks, 2010). A better under standing of attributes of patient-centered care and areas for improvement is needed in order to develop nursing policies that in - crease the use of this model in health care settings. The purpose of this discussion is to clarify the concept of patient-cen- tered care for consistency with the common understanding about pa - tient satisfaction and the quality of care delivered from nurses to patients. Attributes from a customer service model, the Gap Model of Service Quality, are used in a focus on the perspective of the patient as the driver and evaluator of service
- 3. quality. Relevant literature and the Gap Model of Service Quality (Parasuraman, Zeithaml, & Leonard, 1985) are reviewed. Four gaps in patient-centered care are identified, with discussion of nursing implica- tions. Background and Brief Literature Review Patient-Centered Care The Institute of Medicine (IOM, 2001a) and Epstein and Street (2011) identified patient-centeredness as one of the areas for improvement in health care quality. The IOM (2001b) defined patient-centeredness as …health care that establishes a partnership among practition- ers, patients, and their families (when appropriate) to ensure that decisions respect patients’ wants, needs, and preferences and that patients have the edu- cation and support they require to make decisions and partici- pate in their own care… (p. 7) Charmel and Frampton (2008) defined patient-centered care as …a healthcare setting in which patients are encouraged to be
- 4. actively involved in their care, with a physical environment that promotes patient comfort and staff who are dedicated to meeting the physical, emotion- al, and spiritual needs of patients… (p. 80) In a concept analysis of person- centered care, Morgan and Yoder (2011) defined it as …a holistic (bio-psychosocial- spiritual) approach to delivering care that is respectful and indi- vidualized, allowing negotiation of care, and offering choice through a therapeutic relation- ship where persons are empow- ered to be involved in health decisions at whatever level is desired by that individual who is receiving the care. (p. 3) Of significance in various defini- tions of patient-centered care is the focus on the patient’s needs, patient control, and the interaction between the patient and health care provider. Being patient-centered suggests health care providers adapt their Beverly Waller Dabney Huey-Ming Tzeng The Gap Model of Service Quality is used to clarify the concept
- 5. of patient-centered care. Four possible patient-centered care service qual- ity gaps were identified. Nurse administrators may use these gaps to identify and develop appropriate outcome measures. Instructions for Continuing Nursing Education Contact Hours appear on page 363. November-December 2013 • Vol. 22/No. 6360 services to reflect the goals, needs, and values of the individual patient. The Joint Commission (2010) expected hospital leaders to develop standards to advance effective com- munication, cultural competence, and patient- and family-centered care. Gerteis, Edgman-Levitan, Daley, and Delbanco (1993) identified seven dimensions of patient-cen- tered care needed to improve health care quality: (a) respect for patients’ values, preferences, and expecta- tions; (b) coordination and integra- tion of care; (c) information, com- munication, and education; (d) physical comfort; (e) emotional sup- port and alleviation of fear and anx- iety; (f) involvement of family and friends; and (g) transition and conti- nuity. Communication with pa -
- 6. tients, which is essential to the appli- cation of patient-centered care, facil- itates patient involvement in the planning of treatment (Hunt, 2009). Patient-centered care can influ- ence patient satisfaction, the quality of health care, and possibly a patient’s desire to return to a health care provider for future services (Andrews, 2009; Charmel & Frampton, 2008). Patients are ex pected to accept more financial responsibility for their health care, and they expect value in their health care purchases as they would with any other major pur- chase (Charmel & Frampton, 2008). McCormack, Manley, and Walsh (2008) emphasized the significant role played by health care policy in developing systems and processes in health care institutions that are per- son-centered. The recommendations of the IOM (2001b) and the Agency for Healthcare Research and Quality (2009) to adopt a philosophy of patient-centeredness have encour- aged many institutions across the United States to implement patient- centered models. A comprehensive report on patient-centered care was developed by the Institute for Family-Centered Care and the Institute for Health Care Im prove - ment, from which four key concepts emerged: (a) respect and dignity, (b)
- 7. information sharing, (c) participa- tion, and (d) collaboration (Johnson et al., 2008). Charmel and Frampton (2008) indicated the attributes of patient-centered care need to be clar- ified to facilitate understanding of their inter-relatedness. As part of the promotion of patient-centeredness for quality improvement, clarifica- tion of the concept of patient-cen- tered care is needed (McCormack et al., 2008). Communication The interaction between nurses and patients is central for the effec- tive application of patient-centered care (Hobbs, 2009). Levinson, Lesser, and Epstein (2010) noted communi- cation is fundamental to the delivery of patient-centered care. Nurse- patient communication seeks to increase the nurse’s understanding of the patient’s needs, perspectives, and values. Nurse-patient communi- cation also provides patients with information needed to participate in their care and assists in correcting unrealistic expectations. Patient-cen- tered communication is not simply agreeing to provide information per patients’ requests, nor is it throwing information at patients and leaving them to sort it out (Epstein, Fiscella,
- 8. Lesser, & Stange, 2010). Skillful com- munication with patients helps to build trust and understanding, and may require the clinician to engage in further questioning to explore fully what the patient hopes to achieve. The Joint Commission (2010) emphasized identification of patient communication needs as an issue to be addressed by health care leaders. Patient communication needs may include not only language or hearing barriers, but also emotional or fatigue barriers. In a qualitative study of patients with cancer, Montgomery and Little (2011) found some patients may be unable or even unwilling to express their preferences in regard to treatment during the debilitating stages of health. They suggested patients be assessed indi- vidually for their ability to engage in such communication; some individ- uals may need the health profession- al to assume a greater facilitative role. The quality of relationships and interactions between patients and nurses is of great importance to the achievement of patient-centered care. In addition to adequate infor- mation sharing, structures and processes are needed to enhance the delivery of patient-centered care.
- 9. Delivery of Patient-Centered Care Luxford, Safran, and Delbanco (2011) interviewed senior staff and patient representatives in a qualita- tive study. Several organizational attributes and processes that facili- tate patient-centered care emerged, including the following: (a) strong, committed senior leaders; (b) clear communication of strategic vision; (c) active engagement of patients and families; (d) sustained focus on staff satisfaction; (e) active measure- ment and feedback reporting of patient experiences; (f) adequate resourcing of care delivery redesign; (g) staff capacity building; (h) accountability and incentives; and (i) a culture supportive of change and learning. Barriers included the need to change the organizational culture from a provider-focus orien- tation to a patient-focus one, and the length of time needed for the transi- tion to take place. Patient-centered care delivery can appear superficial and unconvincing if confusion exists about the mean- ing of patient-centered care (Epstein & Street, 2011). Patient-centered behaviors, such as respecting pa - tients’ preferences, should be justifi-
- 10. able on moral grounds alone and independent of their relationship to health outcomes. Berwick (2009) claimed health system design may affirm patient-centered care as a dimension of quality in its own right. Patient-centered care should not be confirmed just through its effect on patient or organizational outcomes. Evidence-base literature about identifying interventions for improved outcomes in patient-cen- tered care is lacking, partially due to unclear conceptual models and gold- standard measures (Groene, 2011). Brief Overview of the Gap Model of Service Quality The Gap Model of Service Quality (Parasuraman et al., 1985) (the Model) is a widely used business model that focuses on the perspectives of cus- November-December 2013 • Vol. 22/No. 6 361 tomers to determine quality and pro- vides an integrated view of the cus- tomer-company relationship. The Model is useful for evaluating patient-centeredness in nursing care because of its focus on the customer’s perspective as a measurement of serv- ice quality. In addition, it facilitates
- 11. the derivation of statements of patient-centered care as an indicator of quality health care. The Model included five unique gaps in service quality that can influence quality as experienced by the customer. Based on earlier reports (Charmel & Frampton, 2008; IOM, 2001a), gaps number 1, 2, 3, and 5 in the Gap Model of Service Quality had similar- ities to the concept of patient-cen- tered care. A brief description of these four gaps follows. Gap 1. Customer expectation vs. management perception gap. This gap, also identified as the knowledge gap, reveals discrepancies between man- agers’ perceptions of customer expectations and the actual expecta- tions of the customers. This gap in service quality occurs because man- agers fail to identify customer expec- tations accurately. The size of the gap depends on upward communication from customer to top management (Parasuraman et al., 1985). Gap 2. Management perceptions vs. service standards gap. This gap, also known as the design gap, measures how well the managers’ perceptions of customer expectations are translat- ed into service design standards. Service design standards are policies and expectations of the way service is
- 12. to be provided. This gap depends on managers’ belief service quality is important and possibly dependent on the resources available for the pro- vision of the service. However, if managers’ initial understanding of customer expectations is flawed, inef- ficient service standards inevitably will be produced (Parasuraman et al., 1985). Gap 3. Service standards vs. service delivery gap. This gap, also referred to as the performance gap, represents discrepancies between service design and service delivery. This gap occurs when the specified policies are not followed in service delivery. The quality of delivered service can be affected by numerous factors, such as skill level, type of training received, deficiencies of human resource policies, failure to match supply and demand, degree of role congruity or conflict, and job fit (Parasuraman et al., 1985). Gap 5. Perceived service vs. expected service gap. This is the gap between customers’ service expectations and their perceptions of the service received. According to Parasuraman and colleagues (1985), customer expectations are based on word-of- mouth communications, personal
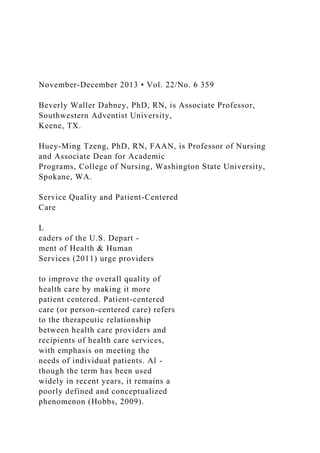
- 13. needs, and past experiences. These four gaps described three key provider abilities and one cus- tomer ability: (a) the ability of man- agers to identify the expectations of their customers correctly, (b) the abil- ity to transfer the identified expecta- tions of their customers into the stan- dards of service, (c) the ability to transform these standards of service into the actual service delivery, and (d) customers’ perception of how the delivered service met their expecta- tions (Parasuraman et al., 1985). Gaps in Patient-Centered Care Based on the Gap Model of Service Quality (Parasuraman et al., 1985), four gaps in patient-centered care were identified (see Figure 1). Each gap depicted in the model of patient-centered care quality in nurs- ing practice is described below. Gap A. Patient expectation vs. nurse perception gap was derived from Gap 1 in the Gap Model of Service Quality. This gap occurs when dis- crepancies arise between nurses’ and nursing administrators’ perceptions of what the patient expects and the patient’s actual expectations. The health care provider fails to identify
- 14. the patient’s expectations accurately. Lack of communication with the patient and an insufficient relation- ship focus are key contributors to this gap. To close this gap, nurses must com- municate with the patient in a way that gathers his or her expectations and needs. Epstein and co-authors (2010) noted the communication goes beyond facts and figures. The cli- nician must frame and tailor informa- tion in response to an understanding of the patient’s concerns, beliefs, and experiences. Aspects of the patient’s culture, past experiences, his or her perceptions from comments made by others, and immediate personal needs all shape what the patient desires and expects from health care services. The key to closing this gap is to reach consensus about an approach to care which is achieved through shared deliberation. Gap B. Nurse and nursing adminis- trator perceptions vs. patient-centered care standards gap was derived from Gap 2 in the Gap Model of Service Quality. This gap depends on the health care provider’s and adminis- trator’s beliefs that patient-centered care is important to quality of care and it is possible to provide patient-
- 15. centered care. This gap is measured by how well the health care delivery design matches the health care provider’s perceptions of the pa - tient’s expectations or needs. Indi - vidual nurses have their own sets of values and service standards based on their backgrounds and what they perceive the patient’s expectations to be. This gap is measured by how well the health care delivery design matches the health care provider’s perceptions of the patient’s expecta- tions or needs. To close this gap, nurse administra- tors must decide that meeting the needs of individual patients is a prior- ity, set organizational standards, and provide resources necessary to meet those standards. Individual nurses must decide if the provision of patient-centered care is a priority. The infrastructure of patient-centered care is supported through the senior nurs- ing team’s commitment to the princi- ples of patient-centered care. How - ever, development of appropriate standards is contingent on identify- ing patient needs correctly. Gap C. Patient-centered care stan- dards vs. delivery of patient-centered care gap was derived from Gap 3 in the Gap Model of Service Quality. This gap represents variations in
- 16. service design and service delivery. The service standards are to be derived from the perceived expecta- tions of patients. Service standards are based on the principles of Service Quality and Patient-Centered Care November-December 2013 • Vol. 22/No. 6362 patient-centered care, and need to be translated to actual delivery of care. Nurses can have great impact on closing this gap. In practice, patient-centered care is not offered consistently due to nursing factors, such as poor staffing, fatigue, burnout, and lack of educa- tion on the delivery of patient-cen- tered care. A qualitative meta-syn- thesis of four studies found evidence of sustained high commitment nec- essary to the development of person- centered cultures in clinical settings (McCormack, Karlsson, Dewing, & Lerdal, 2010). However, other cultur- al characteristics (e.g., the level of staff support) may determine the extent to which that commitment could be sustained. Gap D. Patient expectation of health
- 17. care service vs. patient perception of actual health care service received gap was derived from Gap 4 in the Gap Model of Service Quality. This gap occurs when the patient’s expecta- tions, which are molded by past experiences, culture, personal needs, and word of mouth, are not met or are lacking in some way (Hunt, 2009; Parasuraman et al., 1985). In other words, when care is not patient-centered, patient expecta- tions cannot be met because they are not identified. McCormack and co- authors (2008) suggested a direct relationship between patients’ expe- riences of daily care and their percep- tions of service effectiveness. To close this gap and understand patient preferences, nursing adminis- trators need to promote an interac- tive feedback loop that provides health care providers with a mecha- nism to view care through the eyes of patients and families as well as to link the patients and nursing staff togeth- er (DiGioia et al., 2010). A collabora- tive relationship between health care providers and patients can assist in shaping realistic patient expectations FIGURE 1. The Four-Gap Model of Patient-Centered Care Quality in Nursing Practice
- 18. Quality of Patient-Centered Care in Nursing Practice Patient perceived service Patient expectation Delivery of patient-centered standards Nurse and nursing administrator perception of patient expectation Nurse and nursing administrator transla- tion of perceptions into patient-centered care standards
- 19. Gap B: Nurse and nursing administrator perceptions vs. patient-centered care standards gap Gap D: Patient expectation of health care service vs. patient perception of actual health care service received gap Gap A: Patient expectation vs. nurse perception gap Gap C: Patient-centered care standards vs. delivery of patient- centered care gap November-December 2013 • Vol. 22/No. 6 363 related to patients’ individual health care needs, and minimize false per- ceptions due to lack of understand- ing. A complex series of interactions between nurses and patients elicit
- 20. trust and understanding. Nurses need to use the knowledge gathered from these interactions to adapt a plan of care that reflects individual patient needs. Nursing Implications Nurses may use the four-gap model of patient-centered care qual- ity (see Figure 1) to examine their practice. This approach will provide opportunity to identify gaps as well as develop nursing practice interven- tions to close the gaps indicated in this new model. For example, nurse executives and managers may devel- op appropriate outcome measures to monitor the closeness of each corre- sponding gap (e.g., patient satisfac- tion measures; patient-centered out- comes such as survival, function, symptoms, and health-related quali- ty of life; clinical outcomes such as injurious fall occurrences, nurses’ job satisfaction measures, and intention to quit) (DiGioia et al., 2010, Patient- Centered Outcomes Research, 2013). Future Research The four-gap model of patient-cen- tered care quality in nursing practice needs to be tested. Understanding the nurse-patient relationship and the aspects of communication needed for
- 21. successful outcomes is essential. A focus on patient perspectives assists in capturing cultural, spiritual, and emo- tional needs that otherwise may be missed or overlooked. Future research that captures the degrees of similarity or difference between patient per- spectives and provider perspectives will help identify areas of strengths and weaknesses for improvement. Future research also may explore the links between system issues, such as the effects of nurse staffing on the ability to deliver patient-centered care, and the developmental process of standards and policy for delivery of patient-centered care. Conclusion Four patient-centered care serv- ice quality gaps were identified. Individual patient needs influence expectations, and accurate nurse perceptions of these needs require communication with the patient. Collaboration between nurses and patients is essential to provide bet- ter understanding of patient needs and helps patients understand what to expect realistically from their health care experience. Once pa tient needs have been assessed accurately and understood, poli- cies relevant to the characteristics of the clinical settings can be estab-
- 22. lished to promote patient-centered care. McClelland (2010) claimed understanding the patient perspec- tive of health care services is piv- otal to the development of patient- centered, quality services. The shift of health care from a clinician-cen- tric orientation to a patient-centric one can be challenging to the entire health care team. However, to realize fully the benefits of patient-centered care, nurses must focus on achieving gains in the quality of relationships and inter- actions with patients (Epstein et al., 2010). REFERENCES Agency for Healthcare Research and Quality. (2009). National healthcare quality report. Retrieved from http://ahrq.gov/ qual/qrdr09.htm Andrews, S.M. (2009). Patient family-centered care in ambulatory surgery setting. Journal of PeriAnesthesia Nursing, 24(4), 244-246. doi:10.1016/j.jopan. 2009.05.100 Berwick, D. (2009). What ‘patient-centered’ should mean: Confessions of an extrem- ist. Health Affairs, 28(4), w555-w565. Charmel, P.A., & Frampton, S.B. (2008). Building the business case for patient-
- 23. centered care. Healthcare Financial Management, 62(3), 80-85. DiGioia, A., III, Lorenz, H., Greenhouse, P.K., Bertoty, D.A., & Rocks, S.D. (2010). A patient-centered model to improve met- rics without cost increase: Viewing all care through the eyes of patients and families. Journal of Nursing Admini - stration, 40(12), 540-546. Epstein, R.M., & Street, R.L. (2011). The val- ues and value of patient-centered care. Annals of Family Medicine, 9(2), 100- 103. Epstein, R., Fiscella, L., Lesser, C., & Stange, K. (2010). Why the nation needs a policy push on patient-centered health care. Health Affairs, 29(8), 1489-1495. Gerteis, M., Edgman-Levitan, S., Daley, J., & Delbanco, T.L. (1993). Introduction: Service Quality and Patient-Centered Care Instructions For Continuing Nursing Education Contact Hours Service Quality and Patient- Centered Care Deadline for Submission: December 31, 2015
- 24. MSN J1322 To Obtain CNE Contact Hours 1. For those wishing to obtain CNE con- tact hours, you must read the article and complete the evaluation through AMSN’s Online Library. Complete your evaluation online and print your CNE certificate immediately, or later. Simply go to www.amsn.org/library 2. Evaluations must be completed online by December 31, 2015. Upon comple- tion of the evaluation, a certificate for 1.3 contact hour(s) may be printed. Fees – Member: FREE Regular: $20 Objectives This continuing nursing educational (CNE) activity is designed for nurses and other health care professionals who are interest- ed in service quality and patient-centered care. After studying the information pre- sented in this article, the nurse will be able to: 1. Describe patient-centered care. 2. Discuss gaps in patient-centered care. 3. Explain the nursing implications of using the Gap Model of Service Quality to clar- ify patient-centered care. Note: The authors, editor, and education
- 25. direc tor reported no actual or potential conflict of interest in relation to this continuing nursing education article. This educational activity has been co-provided by AMSN and Anthony J. Jannetti, Inc. Anthony J. Jannetti, Inc. is a provider approved by the California Board of Registered Nursing, provider number CEP 5387. Licensees in the state of CA must retain this certificate for four years after the CNE activity is completed. Anthony J. Jannetti, Inc. is accredited as a provider of continuing nursing education by the American Nurses’ Credentialing Center’s Commission on Accreditation. This article was reviewed and formatted for contact hour credit by Rosemarie Marmion, MSN, RN-BC, NE-BC, AMSN Education Director. Accreditation status does not imply endorsement by the provider or ANCC of any commercial product. November-December 2013 • Vol. 22/No. 6364 Medicine and health from the patient’s perspective. In M. Gerteis, S. Edgman- Levitan, J. Daley, & T.L. Delbanco (Eds.), Through the patient’s eyes: Under - standing and promoting patient-centered care (pp. 1-15). San Francisco, CA: Jossey-Bass.
- 26. Groene, O. (2011). Patient centeredness and quality improvement efforts in hospitals: Rationale, measurement, implementa- tion. International Journal for Quality in Health Care, 23(5), 531-537. Hobbs, J.L. (2009). A dimensional analysis of patient-centered care. Nursing Re - search, 58(1), 52-62. Hunt, M.R. (2009). Patient-centered care and cultural practices: Process and criteria for evaluating adaptations of norms and standards in health care institutions. HEC Forum, 21(4), 327-339. Institute of Medicine (IOM). (2001a). Six aims for improvement. In Crossing the quality chasm (pp. 41-61). Washington, DC: National Academy Press. Institute of Medicine (IOM). (2001b). Executive summary. In M.P. Hurtado, E.K. Swift, & J.M. Corrigan (Eds.), Envisioning the national healthcare qual- ity report (pp. 1-18). Washington, DC: National Academy Press. Retrieved from http://books.nap.edu/catalog.php? record_id=10073 Johnson, B., Abraham, M., Conway, J., Simmons, L., Edgman-Levitan, S., Sodomka, P., … Ford, D. (2008). Partnering with patients and families to design a patient and family centered
- 27. healthcare system. Bethesda, MD: Institute of Family Centered Care. Levinson, W., Lesser, C.S., & Epstein, R.M. (2010). Developing physician communi- cation skills for patient-centered care. Health Affairs, 29(7), 1310-1318. Luxford, K., Safran, D.G., & Delbanco, T. (2011). Promoting patient-centered care: A qualitative study of facilitators and bar- riers in healthcare organizations with a reputation for improving the patient expe- rience. International Journal for Quality in Health Care, 23(5), 510-515. McClelland, H. (2010). Service improvement and patient experience. International Emergency Nursing, 18(4), 175-176. McCormack, B., Karlsson, B., Dewing, J., & Lerdal, A. (2010). Exploring person-cen- teredness: A qualitative meta-synthesis of four studies. Scandinavian Journal of Caring Sciences, 24(3), 620-634. McCormack, B., Manley, K., & Walsh, L. (2008). Person-centered systems and processes. In K. Manley, B. McCormack, & V. Wilson V (Eds), International prac- tice development in nursing and health- care (pp. 17-41). Oxford, England: Blackwell Publishing. Montgomery, K., & Little, M. (2011). Enriching patient-centered care in serious illness: A
- 28. focus on patients’ experiences of agency. The Milbank Quarterly, 89(3), 381-398. Morgan, S.S., & Yoder, L. (2011). A concept analysis of person-centered care. Jour - nal of Holistic Nursing. doi:10.1177/ 0898010111412189 Parasuraman, A., Zeithaml, V., & Leonard, B. (1985). A conceptual model of service quality and its implications for further research. Journal of Marketing, 49(4), 41-50. Patient-Centered Outcomes Research. (2013). Patient-centered outcomes re - search. Retrieved from http://www.pcori. org/research-we-support/pcor/ Scott, A. (2010). Quality lessons. Patient- centered care vital to outcomes, cost. Modern Healthcare, 40(46), 22. The Joint Commission. (2010). Advancing effective communication, cultural compe- tence, and patient- and family-centered care: A roadmap for hospitals. Oakbrook Terrace, IL: Author. U.S. Department of Health & Human Services. (2011). National quality strategy will pro- mote better health, quality care for Americans (press release). Retrieved from http://www.hhs.gov/news/press/ 2011pres/03/20110321a.html
- 29. Copyright of MEDSURG Nursing is the property of Jannetti Publications, Inc. and its content may not be copied or emailed to multiple sites or posted to a listserv without … Palliative Medicine 2016, Vol. 30(3) 224 –239 © The Author(s) 2015 Reprints and permissions: sagepub.co.uk/journalsPermissions.nav DOI: 10.1177/0269216315606645 pmj.sagepub.com What is already known about the topic? •• Early integration of palliative care into the management of patients with serious disease has the potential to both improve quality outcomes for patients and families and reduce healthcare costs. •• Despite these benefits, significant barriers exist in the United States to the early integration of palliative care in the disease trajectory of individuals with serious illness. •• A number of studies have identified and discussed specific barriers to palliative care integration, yet we lack an organized synthesis of the data on barriers to palliative care integration across domains. Education, implementation, and policy barriers to greater integration of
- 30. palliative care: A literature review Melissa D Aldridge1, Jeroen Hasselaar2, Eduardo Garralda3, Marlieke van der Eerden2, David Stevenson4, Karen McKendrick1, Carlos Centeno3 and Diane E Meier1,5 Abstract Background: Early integration of palliative care into the management of patients with serious disease has the potential to both improve quality of life of patients and families and reduce healthcare costs. Despite these benefits, significant barriers exist in the United States to the early integration of palliative care in the disease trajectory of individuals with serious illness. Aim: To provide an overview of the barriers to more widespread palliative care integration in the United States. Design and data sources: A literature review using PubMed from 2005 to March 2015 augmented by primary data collected from 405 hospitals included in the Center to Advance Palliative Care’s National Palliative Care Registry for years 2012 and 2013. We use the World Health Organization’s Public Health Strategy for Palliative Care as a framework for analyzing barriers to palliative care integration. Results: We identified key barriers to palliative care integration across three World Health Organization domains: (1) education domain: lack of adequate education/training and perception of palliative care as end-of-life care; (2) implementation domain: inadequate size of palliative medicine–trained workforce, challenge of identifying patients appropriate for palliative care referral, and need for
- 31. culture change across settings; (3) policy domain: fragmented healthcare system, need for greater funding for research, lack of adequate reimbursement for palliative care, and regulatory barriers. Conclusion: We describe the key policy and educational opportunities in the United States to address and potentially overcome the barriers to greater integration of palliative care into the healthcare of Americans with serious illness. Keywords Palliative care, barriers, integrated palliative care 1 Department of Geriatrics and Palliative Medicine, Icahn School of Medicine at Mount Sinai, New York, NY, USA 2 Radboud University Medical Center, Nijmegen, The Netherlands 3 ATLANTES Research Programme, Institute for Culture and Society, University of Navarra, Pamplona, Spain and Palliative Medicine Group, Area of Oncology and Haematology, Navarra´s Health Research Institute (IDISNA), Pamplona, Spain 606645PMJ0010.1177/0269216315606645Palliative MedicineAldridge et al. research-article2015 Review Article 4Vanderbilt University School of Medicine, Nashville, TN, USA 5Center to Advance Palliative Care, New York, NY, USA
- 32. Corresponding author: Melissa D Aldridge, Department of Geriatrics and Palliative Medicine, Icahn School of Medicine at Mount Sinai, One Gustave L. Levy Place, Box 1070, New York, NY 10029, USA. Email: [email protected] mailto:[email protected] http://crossmark.crossref.org/dialog/?doi=10.1177%2F02692163 15606645&domain=pdf&date_stamp=2015-09-24 Aldridge et al. 225 What this paper adds? •• Barriers in the education domain are lack of adequate education/training and perception of palliative care as end-of- life care. •• Barriers in the implementation domain are the inadequate size of the palliative medicine–trained workforce, the challenge of identifying patients appropriate for palliative care referral, and the need for culture change across settings. •• Barriers in the policy domain are the fragmented healthcare system in the United States, need for greater funding for research, lack of adequate reimbursement for palliative care, and regulatory barriers, particularly in the nursing home setting. Implications for practice, theory, or policy •• Using the World Health Organization’s Public Health Strategy for Palliative Care framework, the barriers we
- 33. identified may be best addressed with a multipronged approach. •• Expansion of the palliative medicine–trained workforce and greater investment in palliative care research are critical to building the evidence base for palliative care integration and securing funding for palliative care services. •• Establishment of guidelines to “trigger” palliative care consultation may facilitate earlier integration of palliative care for individuals across multiple settings and in varying disease populations. Introduction During the last decade, palliative care has been one of the fastest growing trends in US healthcare. The number of palliative care teams within US hospitals with 50 or more beds has nearly tripled since the year 2000 to more than 1700 programs serving approximately 6 million Americans in 2012.1 This growth has occurred primarily in response to the increasing number of Americans living with serious and chronic illnesses and to the caregiving realities faced by their families. Approximately 90 million Americans are living with serious illness, and this number is expected to more than double over the next 25 years.2 About 20% of all Medicare beneficiaries have five or more chronic condi- tions, and two-thirds of Medicare spending goes to cover their care.3 This patient population is also the most likely to benefit from palliative care. The dominant three palliative care delivery models in the United States are hospital palliative care, community palliative care, and hospice. Hospital palliative care teams either provide consultation to the attending physician or
- 34. assume primary oversight of care, depending on the pref- erences of the referring physician. Consultations occur in the inpatient setting, the intensive care unit (ICU), and emergency department (ED). Community palliative care includes a range of delivery models designed to meet the needs of seriously ill individuals and their families, outside the inpatient or hospital setting. Palliative care may be pro- vided in the patient’s home, a nursing home, an assisted living facility, or an outpatient clinic such as a physician’s office, dialysis unit, or cancer center. These care models are developing rapidly in an effort to meet the needs of the sickest and costliest patients—who may otherwise resort to 911 calls, ED visits, and hospitalizations for problems that could have been addressed safely and effectively in the community. Hospice care is a well-known and compre- hensive delivery model of palliative care, but in the United States, it is limited to terminally ill patients who agree to give up insurance coverage for disease treatment. The Medicare hospice benefit (and those of other payer’s) defines hospice eligibility as appropriate for patients when two doctors certify a prognosis of 6 months to live if the disease follows its usual course, and the patient (or surro- gate) agrees to forgo insurance coverage for disease treat- ment of the terminal illness. The World Health Organization (WHO) considers pal- liative care to be “an approach that improves the quality of life of patients and their families through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual.”4–6 Early integration of palliative care into the overall management of patients with serious disease has the potential to improve quality outcomes for patients and families and to reduce healthcare costs.7–19
- 35. Despite these substantial benefits, there are significant barriers in the United States to the early integration of pal- liative care in the disease trajectory of individuals with serious illness. Our objective is to provide an overview of the barriers to more widespread palliative care integration in the United States. We achieve this objective through a review of existing literature in combination with primary survey data from the Center to Advance Palliative Care (CAPC). We then outline the key opportunities on the US policy agenda for addressing these barriers to greater pal- liative care integration in the United States. Methodology Framework: WHO’s public health model Our analysis uses the WHO’s Public Health Strategy for Palliative Care4 to frame our discussion of barriers to pal- liative care in the United States. The public health model 226 Palliative Medicine 30(3) postulates that in order to effectively integrate palliative care into a society, and change the experience of patients and families, the following components must be addressed: (1) education of healthcare workers and the public, (2) implementation of palliative care services at all levels throughout society, (3) appropriate policies, and (4) ade- quate drug availability. Our analysis will focus on policy, education, and implementation because drug availability is not a significant barrier in the United States to palliative care growth.
- 36. Working definitions We used the following definitions in our discussion of bar- riers to palliative care in the United States: 1. Integrated palliative care. Integrated palliative care involves bringing together administrative, organizational, clinical, and service aspects in order to realize continuity of care between all actors involved in the care network of patients receiving palliative care. It aims to achieve quality of life and a well-supported dying process for the patient and the family in collaboration with all the care givers (paid and unpaid).20 2. Barriers to integrative palliative care. Those that avoid bringing together administrative, organiza- tional, clinical, and service aspects in order to realize continuity of care between all actors involved in the care network of patients receiving palliative care.20 Data sources Our analysis comprised both a review of existing literature, national/government reports, and survey data collected by CAPC. Details regarding these sources are as follows. Literature search. We conducted a literature search of Pub- Med in March 2015. Our search terms included “barriers” and “palliative care,” and we included the literature pub- lished between 2005 and March 2015. We identified a total of 143 publications, and two authors screened the titles and abstracts for applicability. The following publications were excluded: 85 that were internationally based, 20 that were focused on the clinical treatment of patients, 11 that were tangential to the topic of barriers to integrated pallia-
- 37. tive care, 9 that were focused on the pediatric population, and 6 that were opinion pieces. We included an additional four articles and two books identified from the reference lists of included articles (Figure 1). We categorized the lit- erature as either original research, review article, report, or book and indicated the population/setting in which the research was conducted and the type of barrier addressed by the document using the previously mentioned WHO public health model (Table 1). CAPC Registry data. We used primary data collected by the CAPC’s National Palliative Care Registry to exemplify the barriers identified in the literature review. The National Palliative Care Registry collects operational data on pallia- tive care programs to promote standardization and improve the quality of palliative care in the United States and is the only data repository of its kind. The registry has been col- lecting information and reporting back to hospital-based palliative care programs since 2008, and during the past 6 years more than 1000 programs have participated. To be eligible to submit program data to the registry, hospital- based palliative care programs must meet the following eligibility criteria: 1. The palliative care program is part of a formally organized and legally constituted entity that pri- marily provides healthcare services, or a sub-unit Publica�ons iden�fied through database searching (n=143) Addi�onal publica�ons iden�fied through
- 38. other sources (n=6) Publica�ons excluded: Interna�onally focused (n=85) Clinical treatment focused (n=20) Tangen�al to topic area (n=11) Pediatric focused (n=9) Opinion pieces (n=6) Publica�ons included in analysis (n=18) Figure 1. Flowchart of included and excluded publications. Aldridge et al. 227 of a legally constituted entity that may be, but need not be, health related. 2. The palliative care program has been providing palliative care services for at least 1 month. 3. The palliative care program provides care to patients at one or more locations within the broad continuum of care settings (e.g. hospital, home, office, long-term care, hospice, and nurs- ing home). 4. The palliative care program representative(s) act in good faith in providing complete and accurate information reported on the survey.
- 39. This report uses registry data from 2012 to 2013 for 405 hospital-based palliative care programs throughout the United States. Specifically, we report responses from the following survey question: “What resource(s) would be most helpful to you in growing your palliative care program (consult and/or inpatient palliative care unit)?” Results: barriers to palliative care integration in the United States Our literature review resulted in 18 key papers which are summarized in Table 1. The barriers we identified from these papers are described in the following sections and are summarized by the WHO domains below: •• Education-related barriers: || Lack of adequate education and training for medical residents. || Perception of palliative care as end-of-life care by healthcare providers and the public. •• Implementation-related barriers: || Inadequate size of palliative medicine–trained workforce. || Challenge of identifying patients appropriate for palliative care referral. || Need for culture change regarding palliative care across settings. Table 1. Key literature addressing barriers to integrated palliative care in the United States.
- 40. Author name Type Setting/population Barrier category Abrahm21 Review article Patients with cancer Education (training) Aldridge Carlson et al.22 Review article Nursing home setting Policy (regulatory) and implementation (staffing) Dalal et al.23 Original research Patients with cancer Education Fadul et al.24 Original research Medical oncologists Education Feeg and Elebiary25 Original research Healthcare professionals Education Gavazzi et al.26 Original research Patients with heart failure or chronic obstructive pulmonary disease Implementation Goepp et al.27 Original research Healthcare professionals in a hospital setting Policy, implementation, and education Grudzen et al.28 Original research Emergency department Implementation (culture, staffing), education, and policy (legal concerns) Institute of Medicine29 Report Multiple Policy, implementation, and education
- 41. Huskamp et al.30 Review article Nursing home setting Policy, implementation, and education Kamel et al.31 Original research Residents in the ICU setting Education: curricula, courses for professionals, and trainees Kavalieratos et al.32 Original research Patients with heart failure Implementation and education Lamba et al.33 Original research Emergency department Implementation Morrison34 Book Multiple Policy, implementation, and education Meier7 Review article Multiple Policy and education Snow et al.35 Original research Hospital inpatient Education (patient and family) Song et al.36 Original research Transplant centers Education Von Roenn et al.5 Review article Patients with cancer Policy, implementation, and education 228 Palliative Medicine 30(3) •• Policy-related barriers: || Fragmented structure of the US healthcare sys- tem. || Need for greater funding for palliative care
- 42. research. || Lack of adequate reimbursement and incentives for palliative care for complex patients. || Regulatory barriers to greater palliative care integration in the nursing home setting. Education-related barriers to palliative care in the United States The WHO public health model identifies the domain of education-related barriers as curricula, courses for profes- sionals and trainees, expert training, family caregiver training and support, and media and public advocacy. Our literature review identified numerous examples of lack of education and training being a primary barrier to greater palliative care integration in the United States. While pal- liative care is becoming more important in today’s health system, addressing health professionals’ lack of knowl- edge is crucial to more widespread integration. Lack of adequate education and training for medical resi- dents. A number of studies sought to identify the extent of palliative care knowledge of current US medical students or residents across numerous settings. The fairly consistent conclusion was that students in US medical schools had very little to no training in palliative care and did not feel confident to handle situations that required palliative care consultation. For example, one study31 evaluated residents in the ICU setting and surveyed them to assess their knowl- edge, skills, and perceived barriers toward palliative care in the ICU. This study found that the most common bar- rier identified by residents (19%) was discrepancies in
- 43. goals of care between the medical team and patients/ families. In addition, residents reported that a palliative care consult was most commonly obtained when the patient was terminally ill (23%) as opposed to further upstream in the course of illness. The authors suggest that resident teaching should focus on overcoming communi- cation barriers with patients and their families and identi- fying the best method to teach palliative care in the ICU setting. Similarly, a paper regarding the integration of palliative care into comprehensive cancer care recommended greater training of fellows and practicing oncologists in palliative care skills, including communication, and methods of pre- venting and treating compassion fatigue.21 A qualitative study regarding provider perceptions of barriers to inte- grated palliative care similarly found that there was a need for organized educational services that crossed discipli- nary lines.27 Perception of palliative care as end-of-life care by healthcare providers and the public. A number of studies in our review discussed the perception of palliative care in the United States as equivalent to end-of-life care as a major barrier to greater upstream integration of palliative care in patients’ disease course. We considered this as an education-related barrier because it can be overcome with knowledge and understanding of palliative care both through clinical and professional training as well as through public health edu- cation. A recent review5 concluded that the most signifi- cant barrier to the integration of palliative care at all stages in the treatment of patients with cancer is the largely clini- cian perception that it is end-of-life care. The authors noted that an assessment of perceptions and experiences of palliative
- 44. care providers indicated that some health care professionals viewed palliative care as being primarily focused on symptom control for terminal patients and that these professionals saw palliative care as a consideration only after all disease- modifying treatment had ceased.5 They found that these misperceptions were also identi- fied in multiple other studies. One series of studies hypothesized that the perceived association between the names “palliative care” and “hos- pice” was a barrier to early patient referral. The studies aimed to determine whether a service name change from “palliative care” to “supportive care” was associated with earlier referrals of patients to palliative care services. In the first study,24 the authors found that the name “palliative care” was perceived by 140 medical oncologists and mid- level providers as more distressing and reducing hope to patients and families compared with the term “supportive care.” Medical oncologists and mid-level providers sig- nificantly preferred the name “supportive care” and stated that they would be more likely to refer patients on active primary and advanced cancer treatments to a service named “supportive care.” In actual clinical practice, the second study23 found that the name change from “palliative care” to “supportive care” impacted referral rates. In this study, the authors examined the records of 4701 consecutive patients with a first palliative care consultation before and after a name change from “palliative care” to “supportive care” to determine the rate and timing of palliative care referral. They found that after the name change, there were a 41% greater number of palliative care consultations mainly as a result of a rise in inpatient referrals. In the outpatient set- ting, they found a shorter duration from hospital registra-
- 45. tion to palliative care consultation and from advanced cancer diagnosis to palliative care consultation occurred. These results suggest that the perception of palliative care as end-of-life care is a barrier to palliative care integration. Although some debate exists regarding the equivalence of the terms, “palliative care” and “supportive care,”37 both supportive care in cancer and palliative care have their Aldridge et al. 229 own origins, history, and background and may be primary, secondary, or tertiary.38 In current practice, both approaches share mutual interests that have the potential to stimulate earlier integration in the disease process. A number of studies surveyed physicians in various set- tings regarding barriers to palliative care integration find- ing that the perception of palliative care as end-of-life care was a significant barrier. For example, a survey of 155 physicians caring for patients with lung cancer found that 48% of physicians referred fewer than 25% of their patients for palliative care consultation. A major reason for this low referral rate was concern that a palliative care referral would alarm patients and families.5,39 Similar concerns regarding the expectations of patients and families were voiced in two other studies. In one study, a survey of 74 physicians found that the most commonly endorsed barrier to palliative care referral in the hospital setting was the patient and/or family’s perceived unrealistic expectations regarding disease prognosis.35 In another study summariz- ing barriers to palliative care in the ICU, inflated expecta- tions regarding critical care therapies and preoccupation with an unattainable level of prognostic certainly are two important barriers to earlier palliative care intervention.40
- 46. A study of 74 clinicians across 27 lung transplant centers found that the misconception of palliative care as end-of- life care was a major reported barrier, along with uncer- tainty about patient prognosis and perception that palliative care precludes more aggressive treatment.36 Similarly, sur- vey respondents attending a national palliative care con- ference rated the top three barriers to greater use of palliative care and hospice as (1) physician’s reluctance to make referrals, (2) physician’s lack of familiarity with availability and suitability of hospice, and (3) association of hospice with death.25 These studies illustrate that the misperception of pallia- tive care as end-of-life care and as not compatible with ongoing treatment is a significant barrier to palliative care integration in the United States. To address this barrier, better education about palliative care, for both healthcare providers and the public, could potentially result in greater use and earlier integration of palliative care services for patients with serious illness. These opportunities and ini- tiatives are discussed in the “Options to expand integrated palliative care in the United States” section. Implementation barriers to palliative care in the United States The WHO public health model identifies the domain of implementation-related barriers as those related to opinion leaders, trained manpower, strategic and business plans (including resources and infrastructure), and the existence of standards and guideline measures.4 Our literature review identified a number of significant implementation barriers to greater integration of palliative care in the United States. Inadequate size of the palliative medicine–trained work- force. A major barrier facing the expansion of palliative
- 47. care services in the United States is the lack of palliative medicine–trained physicians, nurses, social workers, and other disciplines. Where there is approximately one cardi- ologist for every 71 persons experiencing a heart attack and one oncologist for every 141 newly diagnosed cancer patients, there is only one palliative medicine physician for every 1200 persons living with a serious or life-threatening illness.41 A recent analysis by the American Academy of Hospice and Palliative Medicine’s Workforce Task Force estimated that the gap between the current supply and the hypothetical demand for hospice and palliative medicine– trained physicians to reach mature staffing levels was 2787–7510 full-time equivalents, which equates to 6000– 18,000 individual physicians, depending on what propor- tion of time each physician devotes to hospice and palliative medicine practice.42 Primary data collected by the CAPC’s National Palliative Care Registry suggest the significance of this barrier to greater integration of palliative care in the United States. Our analysis of the annual program data for years 2012 and 2013 from 405 hospital-based palliative care programs nationwide finds that the barrier most often cited as hampering palliative care program growth is the need for additional staff (Table 2). Registry data show that 80% of programs report the need for funds to hire staff as the number one barrier to palliative care expansion. In addi- tion, even when funds are available to hire palliative med- icine–trained professionals, 26% of programs report difficulty recruiting appropriate staff to already funded but open positions, also a significant barrier to the expansion of their program. Analyses of registry data from years 2012 and 2013 also show that higher staffing levels in hospital-based pal- liative care programs are a key determinant of higher pal-
- 48. liative care penetration in the hospital (i.e. serving more patients in need).1 Figure 2 shows the mean palliative care service penetration for palliative care teams, from the low- est to the highest quartiles in terms of staffing. In addition to the hospital setting, a recent study22 of bar- riers to greater palliative care integration in the nursing home setting found that the most immediate barrier to improving access to palliative care in nursing homes is inadequate training and numbers of staff. Nursing homes face a significant labor shortage and high turnover because of the difficulty of the work, inadequate pay, low respect, and demanding paperwork and regulatory requirements.43,44 The adequacy of nursing home staffing is a significant issue in the United States, and strong evidence supports the relationship between increases in nurse staffing ratios and avoidance of critical quality of care problems.45 Nursing homes tend to have lower proportion of registered nurses (RNs) than other healthcare settings,43 and RNs working in nursing homes often have administrative and supervisory 230 Palliative Medicine 30(3) duties and deliver little direct patient care. It has been sug- gested that a stronger physician presence and oversight of physicians trained in palliative care are needed to improve access and quality of palliative care in the nursing home setting.44 There are two principal reasons for the shortage of palliative medicine providers across disciplines and set- tings. First, palliative medicine is a new specialty, for- mally recognized in 2007. Thus, although the number of training programs is increasing, as of 2014 there were
- 49. only 115 Accreditation Council for Graduate Medical … International Journal of Palliative Nursing 2015, Vol 21, No 3� 109 © 2 01 5 M A H ea lth ca re L td Abstract Introduction: Effectively discussing palliative care with patients and families requires knowledge and skill. The purpose of this study was to determine perceived needs of inpatient nurses for communicating with patients and families about palliative and end-of-life (EoL) care.
- 50. Method: A non-experimental design was used. In total, 60 inpatient nurses from one hospital in Idaho completed the End of Life Professional Caregiver Survey (EPCS), which examines three domains: patient and family-centered communication, cultural and ethical values, and effective care delivery. Results: The number of years’ experience nurses had (F(9,131.57)=2.22, p=0.0246; Wilk’s ^=0.709) and the unit they worked on (F(6,110)=2.49, p=0.0269; Wilk’s ^=0.775) had a significant effect on their comfort discussing EoL and palliative care with patients and their families. For all three domains, years of nursing experience was positively associated with comfort in communicating about EoL care. Oncology nurses were most comfortable with regard to patient and family-centered communication. Discussion: The success and sustainability of this service is dependent on education for health-care providers. Studies are needed to determine the most effective ways to meet this educational challenge. Key words: Palliative care l End-of-life care l End-of-life Professional Caregiver Survey l Patient-centered nursing This article has been subject to double-blind peer review. Review of the literature and the authors’ experiences have revealed that inpatient staff nurses may not be prepared to pro- vide optimal end-of-life (EoL) and palliative care to patients and their families (Chan and Webster, 2013; Patel et al, 2012; Prem et al, 2012; Agustinus and Chan, 2013). Palliative care patients can continue to seek curative treat- ments while evaluating their goals and care needs. EoL care patients are usually no longer
- 51. receiving aggressive curative treatment, instead they are receiving comfort care only. In the US, the word ‘hospice’ is interchangeable or synony- mous with EoL care. These patients usually die at home or in the intensive care unit, limiting the contact a regular staff nurse may have in providing care for them. Nurses who are skilled and comfortable in communicating with patients and families about EoL (hospice) and palliative care may improve the quality of life for these patients in the hospital setting. Some patients will make the transition from curative-based care to hospice care during a hos- pital stay. Whether the transition is made smoothly and gradually, depends on the kind of communication and education patients receive from doctors, nurses, and other caregivers while in the hospital (Adams, 2005; Beck et al, 2012; van Brummen and Griffiths, 2013). Palliative care options should be provided to patients in a way that helps them understand the goals and how it differs from EoL care. However, many people opt for palliative care only when they are very close to the end of their lives (Raijmakers et al, 2011; Wilson et al, 2011). It seems reasonable to assume that a lack of education and accompanying uneasiness among clinical nurses in discussing palliative care with patients and their families may negatively impact the transition from curative-based care to hospice care. The current research focused on the role of the nurse during the transition in patients’ lives from curative to palliative care. The study aim was to determine the perceived
- 52. educational needs of inpatient staff nurses in the authors’ facility when communicating with patients and families about palliative and EoL care. Methods A non-experimental survey design was used to examine differences based on the age of the nurse, years of nursing experience, and the unit on which he/she worked. End-of-Life Professional Caregiver Survey (EPCS) To measure educational needs among nurses with regard to communicating about palliative and EoL care and their current degree of com- fort in caring for this patient population, the Research Communicating with patients and their families about palliative and end-of-life care: comfort and educational needs of nurses Cheryl Moir, Renee Roberts, Kim Martz, Judith Perry and Laura J Tivis Cheryl Moir, Home Care/Hospice, Care Coordinator, St. Luke’s Health System, Boise, Idaho, US; Renee Roberts, Clinical Nurse, Bone Marrow Transplant, University of
- 53. Colorado Hospital, Aurora, Colorado, US; Kim Martz, Assistant Professor, Boise State University, Idaho, US; Judith Perry, Home Care/Hospice, Nurse Practitioner, St. Luke’s Health System, Boise, Idaho, US; Laura Tivis, Nursing Research Director, St. Luke’s Health System, Boise, Idaho, US Correspondence to: Cheryl Moir [email protected] 110� International Journal of Palliative Nursing 2015, Vol 21, No 3 Research © 2 01 5 M A H
- 54. ea lth ca re L td End-of-Life Professional Caregiver Survey (EPCS) was used in this study. The EPCS was distributed to a convenience sample of clinical nurses working exclusively in telemetry, oncol- ogy and critical care units (Lazenby et al, 2012). Permission to use the EPCS was granted by the survey designers. The EPCS is a 28-item, psy- chometrically valid scale developed to assess the palliative and EoL educational needs of profes- sionals, and was validated in a large study encompassing doctors, nurses and social work- ers (Lazenby et al, 2012). For each item, a 5-point Likert-style scale was presented (range: not at all to very much). Items represent care- provider comfort and skill with a variety of situ- ations related to palliative and EoL care (e.g. ‘I am comfortable helping families to accept a poor prognosis’). Higher scores indicate greater skill or comfort and skill. Three distinct factors were identified by Lazenby et al (2012): (1) patient and family-centered communication (PFCC), (2) cultural and ethical values (CEV), and (3) effective care delivery (ECD) (Lazenby et al (2012: 429). Data collection
- 55. Data were collected over a 1-month period in 2013. The survey was conducted at a 378-bed hospital in Idaho. Telemetry, oncology, and criti- cal care units were chosen because patients on these units were most often among those transi- tioning from curative-based care to EoL care. The three units employed a combined clinical nursing staff of approximately 215 (telemetry unit 90, oncology 35, and critical care 90). Recruitment emails were sent to 175 clinical nurses (identified from the 215 as having active email addresses) employed on the designated units, requesting participation in the research project. In addition, recruitment flyers were posted on the selected units to inform nurses of the project and request participation. Both online and handwritten survey options were available, and both options were anony- mous. Handwritten surveys were made available on each of the telemetry, oncology and critical care units in the hospital. An investigator- addressed envelope was attached to each paper survey for nurses to return the completed instru- ment through the hospital’s internal mail system to retain anonymity. The handwritten surveys were kept in a locked office and shredded after data collection was complete. The online survey was hosted by REDCap (Research Electronic Data Capture) at the University of Washington, Institute of Translational Health Sciences (https:// www.iths.org/). Ethical considerations Data collection began following approval from
- 56. the hospital Institutional Review Board (IRB). Permission to distribute the survey was also acquired from individual unit managers prior to distribution. Data analysis and results In total, 60 nurses participated in the survey. Based on the number of active email addresses within the three units, this reflects a 34% participation rate. Data were analysed using SAS 10.0 software. Descriptive statistics and Chi-Square were used to analyse demographic information. PFCC, DEV and ECD domain scores were calculated as described by Lazenby et al (2012). Mulitvariate analysis of variance (MANOVA) was used to determine overall effects of age of the nurse, unit the nurse works in, and years of nursing experience across domain scores. Duncan’s Multiple Range Test was used to conduct post-hoc comparisons to determine within-domain differences. Sample distribution across the units was roughly even, with about 37% of respondents were from critical care units, 26% from oncology units, and 37% from telemetry units. The majority of respondents were under 50 years of age: 41% were younger than 30 years, 43% were between 30 and 49 years, and only 16% were 50 years or older. Participant age did not differ between the hospital units included (likelihood ratio χ2(6, n=58) =5.68, p=0.46). Most of the respondents had 2–10 years of nursing experience: 12% had less than 2 years, 33% had 2–5 years, 29% had 5–10 years, and
- 57. 27% had more than 10 years’ experience. In all, years of experience did not significantly differ between work units (likelihood ratio χ2(6, n=60) =9.98, p=0.13). MANOVA revealed that there was an overall effect of experience and unit, but no effect of age [Experience: F(9,131.57)=2.22, p=0.0246; Wilk’s ^=0.709; Unit: F(6,110)=2.49, p=0.0269; Wilk’s ^=0.775; Age: F(9,126.7)=1.19, p=0.3083; Wilk’s ^=0.821]. In contrast to the effect of years of experience on comfort level, only the PFCC domain revealed differences by unit. Oncology nurses reported sig- nificantly higher comfort levels than critical care or telemetry nurses with regard to patient and family-centered communication (see Table 1). Discussion The transition to palliative and/or EoL care can be difficult for patients and their families. During this transition, they may have many questions as they sort through the emotional and logistical aspects ❛ Palliative care options should be provided to patients in a way that helps them understand the goals and how it differs from
- 58. EoL care.❜ International Journal of Palliative Nursing 2015, Vol 21, No 3� 111 Research © 2 01 5 M A H ea lth ca re L td of the situation. Questions might include: What is the difference between palliative and EoL care? How does one access these services? What can one expect from them? In order to answer these ques- tions, health-care staff must possess a basic knowl- edge of palliative and EoL care. Overall, the data suggest that the nurses in this
- 59. study self-report a moderate to high comfort level with their skills in the areas assessed by the EPCS, with more experienced nurses scoring higher than those with less nursing experience.Oncology nurses scored highest in all domains and signifi- cantly higher than their telemetry counterparts, on the PFCC domain. This likely reflects their greater degree of experience communicating with patients and their families about palliative and EoL care options, validating both the instrument and the nurse populations in our study. Scores were lowest within the ECD domain, suggesting that all nurses, across patient popula- tion areas, may benefit from EoL care education in order to increase their own skill and comfort in caring for these patients. ECD items focus on familiarity with palliative and EoL care, effective- ness at helping in EoL patient situations, and resource availability (Lazenby et al, 2012). Anecdotally, several nurses reported to the study team members that they thought EoL education would benefit them in communicating with patients and their families. Future research This study demonstrated that the less experi- enced nurses expressed some discomfort in com- municating with patients at the end of life and their families. Hence, the authors suggest that further exploration of educational needs among staff nurses regarding palliative and EoL care is required. This exploration may lead to the devel- opment of educational interventions designed to increase nurses’ comfort in speaking to patients and their families. Therefore future studies
- 60. should focus on assessing specific educational needs of non-oncology clinical nurses. These nurses are unlikely to routinely care for EoL patients and may not understand the dilemma patients and their families face when transition- ing from palliative to EoL care. Palliative care and EoL patients are found in hospital and community settings; therefore, any educational intervention should include health providers in outpatient areas and especially in home-care services. Limitations There were several limitations to this study. First, the sample was relatively small (despite repre- senting one-third of nurses in the three areas of interest). While a 30% response rate seems rea- sonable, internal employee surveys can be much higher (EngagedMetrics, 2013; CustomInsight, 2014; Surveygizmo, 2014). However, because this was a voluntary research study of nurses, under- taken by nurses, and not an employer-initiated engagement-type survey, response rates in the 80–90% range are not reasonable or expected. Even so, the results of this study may not be gen- eralisable and should be interpreted with caution. Another limitation to this study was the restricted population of nurses who participated (i.e. all were from one hospital). A final limitation to this study is a small data collection flaw within the demographic portion Table 1. Comfort level by unit
- 61. Domain Unit nurses work on Mean comfort level ± SD (Duncan Grouping) Number of participants Patient and family- centered communication (PFCC) Oncology 4.18 ± 0.50 (A) 16 Intensive care unit (ICU)/critical care unit (CCU) 3.96 ± 0.46 (A,B) 22 Telemetry 3.76 ± 0.70 (B) 22 Cultural and ethical values (CEV) Oncology 3.67 ± 0.67 (A) 16
- 62. ICU/CCU 3.69 ± 0.59 (A) 22 Telemetry 3.32 ± 0.83 (A) 22 Effective care delivery (ECD) Oncology 3.53 ± 0.54 (A) 16 ICU/CCU 3.18 ± 0.64 (A) 22 Telemetry 3.18 ± 0.77 (A) 22 Within each domain, means with the same letter are not significantly different. Table 2. Comfort level by years of experience Domain Experience (years) Mean comfort level ± SD (Duncan Grouping) Number of participants Patient and family- centered communication (PFCC) < 2 3.42 ± 0.33 (C) 7
- 63. 2–5 3.77 ± 0.65 (B,C) 20 5–10 4.03 ± 0.44 (A,B) 17 >10 4.31 ± 0.48 (A) 16 Cultural and ethical values (CEV) < 2 3.00 ± 0.60 (C) 7 2–5 3.28 ± 0.80 (B,C) 20 5–10 3.75 ± 0.51 (A,B) 17 >10 3.92 ± 0.59 (A) 16 Effective care delivery (ECD) < 2 2.79 ± 0.37 (B) 7 2–5 3.18 ± 0.87 (A,B) 20 5–10 3.33 ± 0.49 (A) 17 >10 3.55 ± 0.58 (A) 16 Within each domain, means with the same letter are not significantly different.
- 64. 112� International Journal of Palliative Nursing 2015, Vol 21, No 3 Research © 2 01 5 M A H ea lth ca re L td of the information collected. Specifically, hand- written respondents were asked to indicate their years of nursing experience: less than 2 years, 2–5 years, 5–10 year, or >10 years. Post-hoc, the investigators became aware that those with five years of experience may have chosen 2–5 or 5-10 years. No feedback was received with regard to this issue to suggest which category individuals with 5 years of experience chose. Because the study was anonymous, there was no way to re-survey the respondents in order to
- 65. ascertain the correct category for this subgroup. As Table 2 shows, the domain scores did not differ for those with 2–5 years and 5–10 years. It is possible that there may have been differ- ences if the categories had been designed with exclusivity (e.g. 2–5, 6–10). Implications and conclusions This study has important implications around the need for enhanced communication with patients and their families about palliative and EoL care, particularly among less-experienced nurses and those not working in oncology units. The transi- tion point from curative to palliative care can be a challenging time for nurses and patients. Nurses developing skills and knowledge in this area will enable them to help patients and their families make smoother transitions. This study shows a moderate level of perceived skill, with a stronger need for additional knowledge among those nurses with less experience both in terms of years as a nurse and patient population. Understanding the best way to develop that edu- cation is an important subject for future researchers. The authors concluded that additional educa- tion for less experienced nurses could increase comfort levels in all domains and improve care for EoL patients. Going forward, the survey used in this study will be applied to home-health nurses to assess their level of comfort with palliative care patients on their service. Using the responses from the survey, online educational modules will be devel-
- 66. oped by an inter-professional committee to address basic palliative nursing care areas identi- fied by survey participants as an area of educa- tional need. Palliative and EoL care will expand and move beyond hospitals to home-based care, long-term care and other community settings. The success and sustainability of this service will be dependent upon meaningful training of all health-care pro- viders. Further studies will be needed to determine how best to meet this educational challenge. Acknowledgments The authors wish to thank Mr. Rick Tivis (Biostatistician), Mr. David Kent (4S Oncology Director) and Ms. Mary Lou Long (Home Care/Hospice former Director) for their con- tributions to this work. Special thanks to Mr. Danh Nguyen, Nursing Student Research Assistant. We also wish to acknowledge the support of the Institute of Translational Health Sciences (ITHS; grant UL1TR000423 from NCRR/NIH). Declaration of interests The authors have no conflicts of interest to declare. Adams M (2005) Patient and care satisfaction with palliative care services: A review of the literature. ACCNS Journal for Community Nurses 10(2): 11–4 Agustinus S, Chan SWC (2013) Factors affecting the attitudes of nurse towards palliative care in the acute and long term care setting: a systematic review. JBI Library of Systematic Reviews and Implementation Reports 11(1), 1–69 Beck I, Tornquist A, Brostrom L, Edberg AK (2012) Having to
- 67. focus on doing rather than being: nurse assistants’ experi- ence of palliative care in municipal residential care settings. Int J Nurs Stud 49(4):455–64 Chan R, Webster J (2013) End-of-Life pathways for improv- ing outcomes in caring for the dying. Cochrane Database Syst Rev 11:CD008006. doi: 10.1002/14651858. CD008006.pub3 CustomInsight (2014) Increase response rates on employee surveys. http://tinyurl.com/n4bhts6 (accessed 9 March 2014) EngagedMetrics (2013) Employee Survey Average Response Rates. http://tinyurl.com/kccox8a (accessed 2 March 2015) Lazenby M, Ercolano E, Schulman-Green D, McCorkle R (2012) Validity of the end-of-life professional caregiver survey to assess for multidisciplinary educational needs. J Palliat Med 15(4): 427–31 Patel B, Gorawara-Bhat R, Levine S, Shega JW (2012) Nurs- es’ attitudes and experiences surrounding palliative seda- tion: components for developing policy for nursing profes- sionals. J Palliat Med 15(4): 432–7 Prem V, Karvannan H, Kumar SP et al (2012) Study of nurses’ knowledge about palliative care: a quantitative cross-sec- tional survey. Indian J Palliat Care 18(2): 122–7 Raijmakers NJ, van Zuylen L, Costantini M et al (2011) Is- sues and needs in end-of-life decision making: an interna- tional modified Delphi study. Palliat Med 26(7): 947–53 Surveygizmo (2014) Survey response rates. http://tinyurl.com/ ycworuj (accessed 2 March 2015)
- 68. van Brummen B, Griffiths L (2013) Working in a medicalised world: the experience of palliative care nurse specialists and midwives. Int J Palliat Nurs 19(2): 85–91 Wilson F, Gott M, Ingleton C (2011). Perceived risks around choice and decision making at end-of-life: a literature re- view. Palliat Med 27(1): 37–53 ❛ ... any educational intervention should include health providers in outpatient areas and especially in home-care services.❜ Correspondence International Journal of Palliative Nursing welcomes correspondence relating to any of its content, whether only for the Editor’s attention or for publication in the journal. We also encourage letters on any relevant aspects of palliative care from authors who would like to communicate with the readership without necessarily wanting to publish a full-length article. To submit correspondence or discuss the publication potential of a piece, please contact the Editor: [email protected] Copyright of International Journal of Palliative Nursing is the property of Mark Allen
- 69. Publishing Ltd and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.