Downloaded 1,549 times



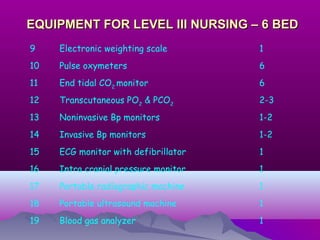
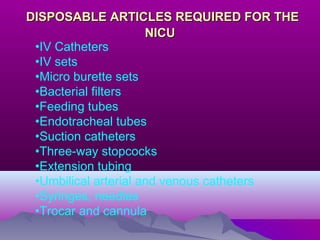
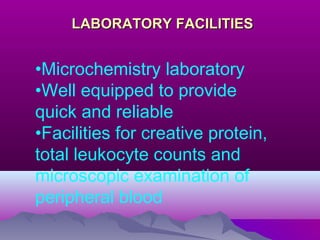
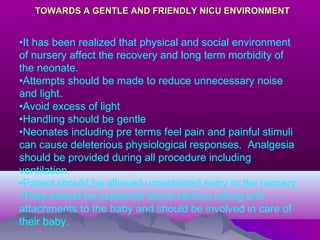



The document discusses the organization and setup of a Neonatal Intensive Care Unit (NICU). It describes the necessary physical space, facilities, equipment, staffing, and organization of care into three levels - basic, high-level, and intensive care. Key requirements for the NICU include appropriate space per bed, ventilation, lighting, environmental controls, and isolation rooms. Staffing must include neonatologists, nurses, and other medical experts. A full range of life-saving equipment is also needed to provide different levels of neonatal care for critically ill newborns.



























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




