Downloaded 55 times

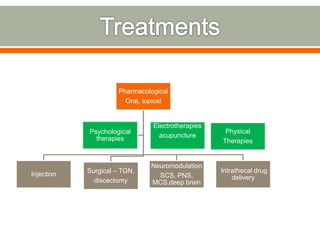
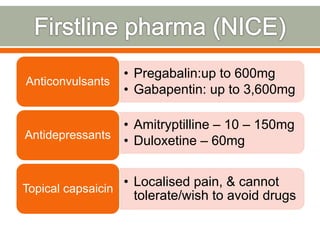
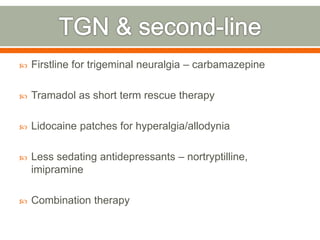
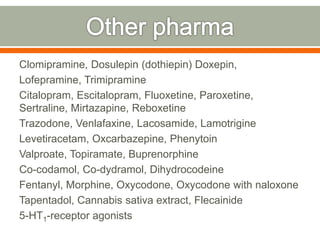


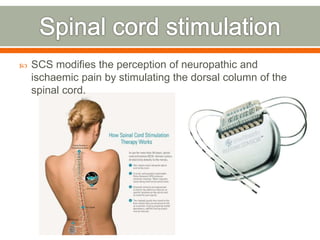






The document discusses various types of neuropathic pain, their causes, symptoms, and current best practices for management, including pharmacological and non-pharmacological treatments. It highlights the emotional impact of chronic pain on patients, the effectiveness of therapies such as spinal cord stimulation and action potential simulation therapy (APS), and reviews recent research findings on pain relief methods. The document also emphasizes the importance of tailored treatment approaches and the potential benefits of alternative therapies in improving quality of life for individuals suffering from chronic pain.





























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





