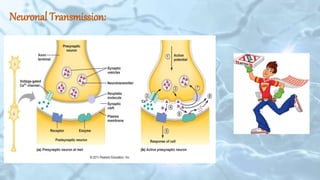
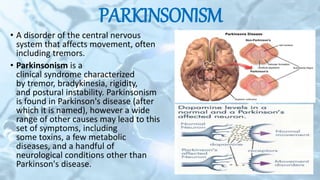
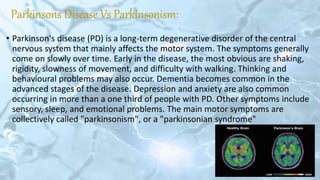
This document discusses Parkinson's disease and related conditions. It begins with an overview of the brain and neuronal transmission. It then defines Parkinsonism and distinguishes it from Parkinson's disease. The document discusses the diagnosis and treatment of Parkinson's disease as well as Parkinson-plus syndromes. It provides clinical clues to differentiate various conditions and discusses their treatment approaches. The document concludes with key points and references.