This document discusses the principles and types of neuromuscular monitoring. It describes the goals of neuromuscular monitoring including quantitative assessment of blockade. It outlines the types of nerve stimulation including electrical and magnetic, and discusses commonly used nerve-muscle units like the ulnar nerve-adductor pollicis. Patterns of nerve stimulation are covered like train-of-four, double burst, and post-tetanic count. Objective monitoring techniques like acceleromyography and mechanomyography are also summarized. Finally, the document evaluates recorded evoked responses with depolarizing and non-depolarizing neuromuscular blocking agents.
Goals
Principles
Typesof neuromuscular monitoring
Definitions
Sites of nerve stimulation and responses
Patterns
Clinical practice
3.
PRINCIPLES
Supra-maximal stimulation:the electrical stimulus required to block all the
muscle fibers of a muscle which are supplied by a single nerve,is the maximum
stimulus. Supra-maximal stimulus is 15 to 20 percent greater than the maximal
stimulus.
Calibration: It adjusts the gain f the device to ensure that the observed response is
within the measurement window of the device and is closest to 100% of control
response.
Impedance: is the resistance offered by the skin to the passage of current. Value =
5 kilo ohms.
Safety margins: neuromuscular block is evident only once 70% of the receptors
are blocked. So, this should be kept in mind 70 % of the receptors may still be
blocked and not detectable on the nerve stimulator.
4.
Types of peripheralnerve stimulation
Electrical
Commonly used in clinical practice
Easy to use
painful
Magnetic
Not used clinically
Bulky apparatus
Not painful
5.
Site of nervestimulation selection
The site should be easily accessible.
Allow quantitative monitoring.
Direct muscle stimulation should be avoided.
Happens when electrodes are directly placed on the muscle being tested.
To prevent this, the nerve-muscle unit should be chosen so that the site of nerve and site
of responding muscle are anatomically distinct.
6.
Nerve-Muscle Units
Ulnarnerve--adductor pollicis muscle.
Easily accessible
When arms are abducted and patient is supine.
Nerve and muscle are topographically distinct.
Adduction of the thumb.
Facial Nerve--orbicularis oculi; Facial Nerve—Corrugator supercilli
When arms are tucked under drapes.
Risk of direct muscle stimulation is significant.
Can be elicited with lower current i.e 23 to 30 mA.
winking of eye and wrinkling of the brow respectively.
7.
Nerve-Muscle Units
PosteriorTibial Nerve—Flexor halluces brevis
Easily accessible
When hands are inaccessible.
Nerve and muscle are topographically distinct.
Flexion of big toe.
8.
Electrodes and assembly
Two types of electrodes are used:
needle
surface
Surface electrode:
pre-gelled silver or silver chloride
Conduction area should be 7 to 11 mm
Negative terminal is placed on nerve
Positive terminal is placed proximally
Space between the centre of two electrodes should be 3 to 6cm.
9.
Electrodes and assemblycontt.
Needle electrodes
Used when skin electrodes cannot be applied
When the selected current cannot be delivered with surface electrodes
Specially coated needles or ordinary injection needles can be used
Sterile technique is mendatory
Needle is placed subcutaneously to avoid direct injury to the nerve.
10.
Patterns of NerveStimulation
Single Twitch
Train Of Four
Train Of Four Ratio
Double Burst
Tetanic Stimulation
Post-tetanic Count Stimulation
11.
Single Twitch Stimulation
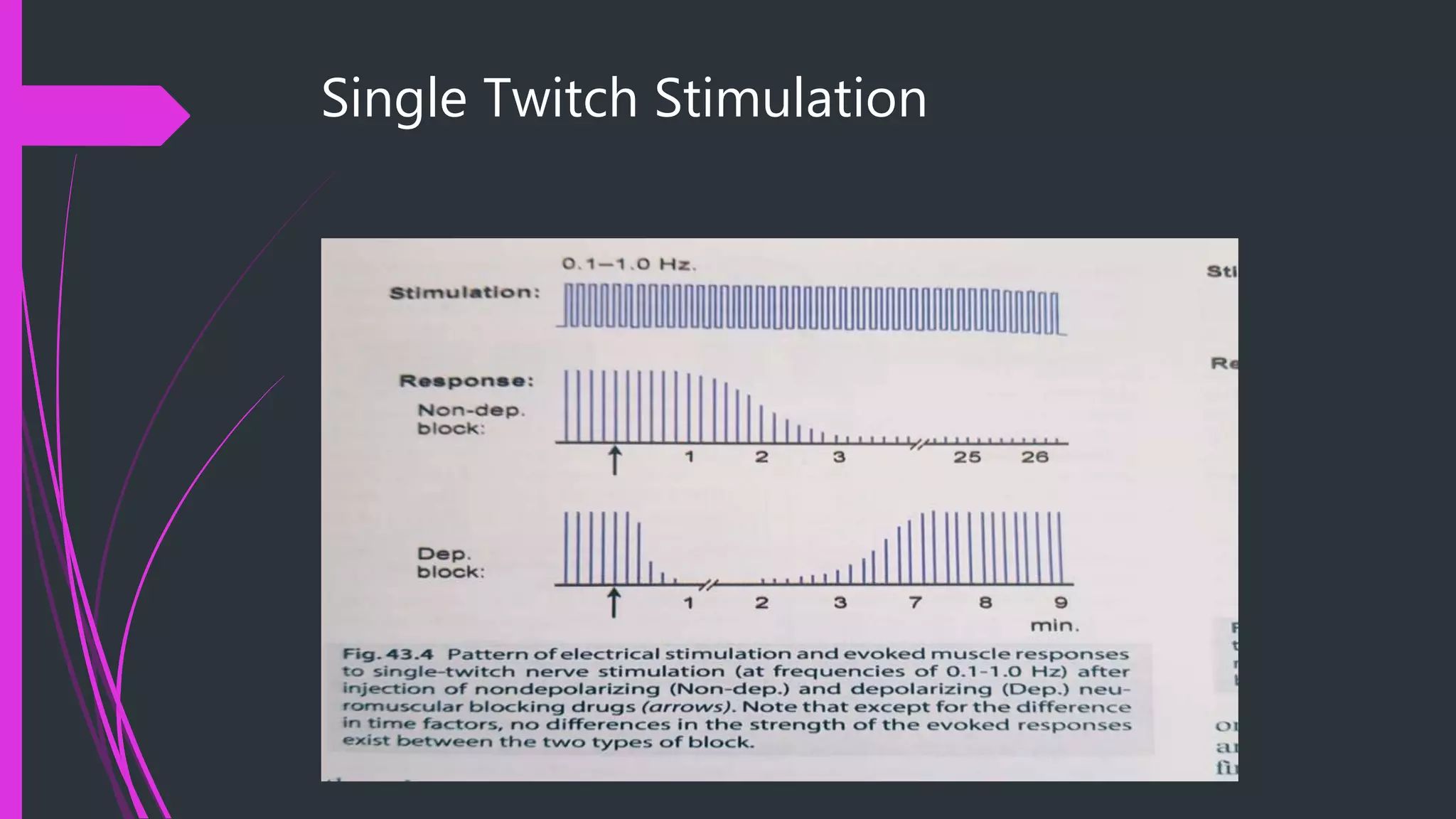
Stimulation Pattern
Single electrical stimulus is applied to the peripheral motor nerve.
Frequency 1hz (once every sec) to 0.1Hz (one every 10 seconds).
Clinical application
Only pattern used to assess the neuromuscular block with depolarizing NMBA
succinylcholine.
As a component of PTC stimulation.
As 0.1 Hz single twitch stimulation, sometimes used in the clinical trials to see the onset
of neuromuscular blockade.
Train Of FourStimulation
Stimulation Pattern
Consists of four supra-maximal stimuli given every 0.5sec (2Hz); and each stimulus in TOF
causes the muscle to contract.
The response evaluation is based upon either of two:
TOF Count: No. of discernible responses after TOF simulation i.e TOF Count.
TOF Ratio: Fade in TOF responses i.e dividing the amplitude of fourth response to that of 1st
response.
1. Without NMBA: all four responses are same---TOF ratio is 1.
2. With Non-dep NMBA:TOF ratio decrease---fade occurs.
3. With Dep NMBA:No Fade occurs---TOF Ratio is 1. Phase 1 block.
4. Fade with dep NMBA: phase II block has occurred.
Train Of FourStimulation
Advantages:
Most frequently used.
Less painful than DBS and PTC.
Reliable for all phases of anesthesia(onset of neuromuscular blockade till recovery).
Limitations:
Subjective assessment overestimates the neuromuscular recovery i,.e. TOF ratio 0.4 to 0.9 fade
cannot be detected either visually or tactically.
TOF ratio does not allow the clinician to quantify intense and deep levelsof neuromuscular
blockade.
Does not allow monitoring of depolarizing neuromuscular blockade.
17.
Double-Burst Stimulation
StimulationPattern:
Two short burst of 50 Hz of tetanic stimulation separated by 750ms, with a 0.2 ms
duration of each square wave impulse in the burst.
Modes of DBS: depend upon the no. of impulses in each burst.
DBS 3,3 Mode: three impulses in each burst
DBS3,2 Mode: 1st burst has 3impulses and second burst has 2 impulses.
Each impulse is of 0.2 second regardless ofDBS mode.
Double-Burst Stimulation
Response:
The individual twitches in each burst are blended and felt to be single amplified muscle
contraction.
The response is two short muscle contractions and fade in second burst compared to the
first burst is the basis for evaluation.
20.
Double-Burst Stimulation
Clinical application
Manual (tactile or visual) detection of block.
Recovery
Post-op residual block.
Advantages vs disadvantages:
Better visal assessment cpmpared to TOF count.
Objective monitoring is superior to DBS.
DBS is painful as compared to TOF.
21.
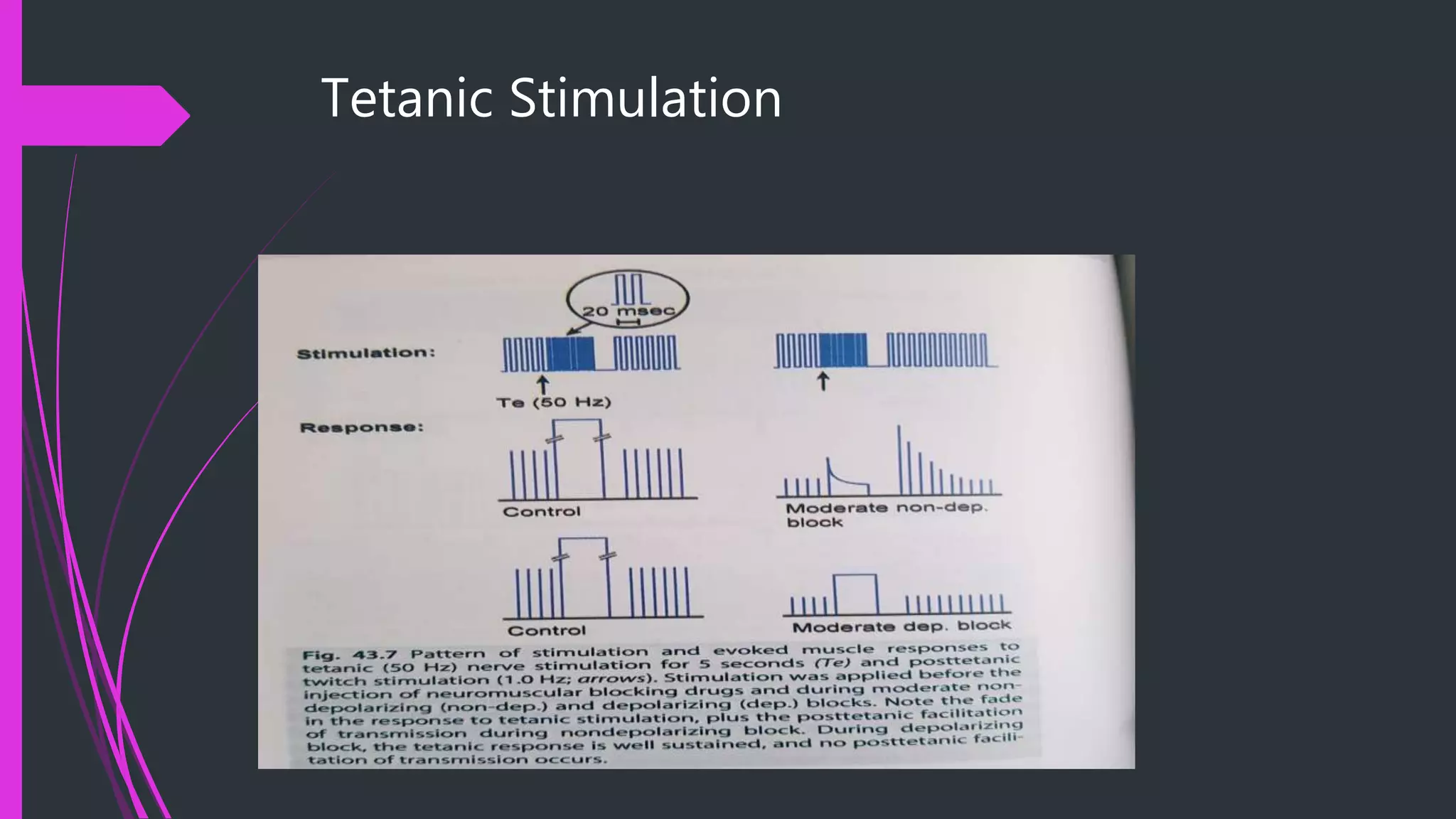
Tetanic Stimulation
StimulationPattern
High frequency delivery of electrical stimuli i.e. 50 Hz for 5 seconds or 100 Hz to 200 Hz
given for 1second.
Response
Without any NMBD: fade does not occur.
With non-dep NMBD: fade occurs.
With Dep NMBD: no fade.
Fade with Dep NMBD: phase II block.
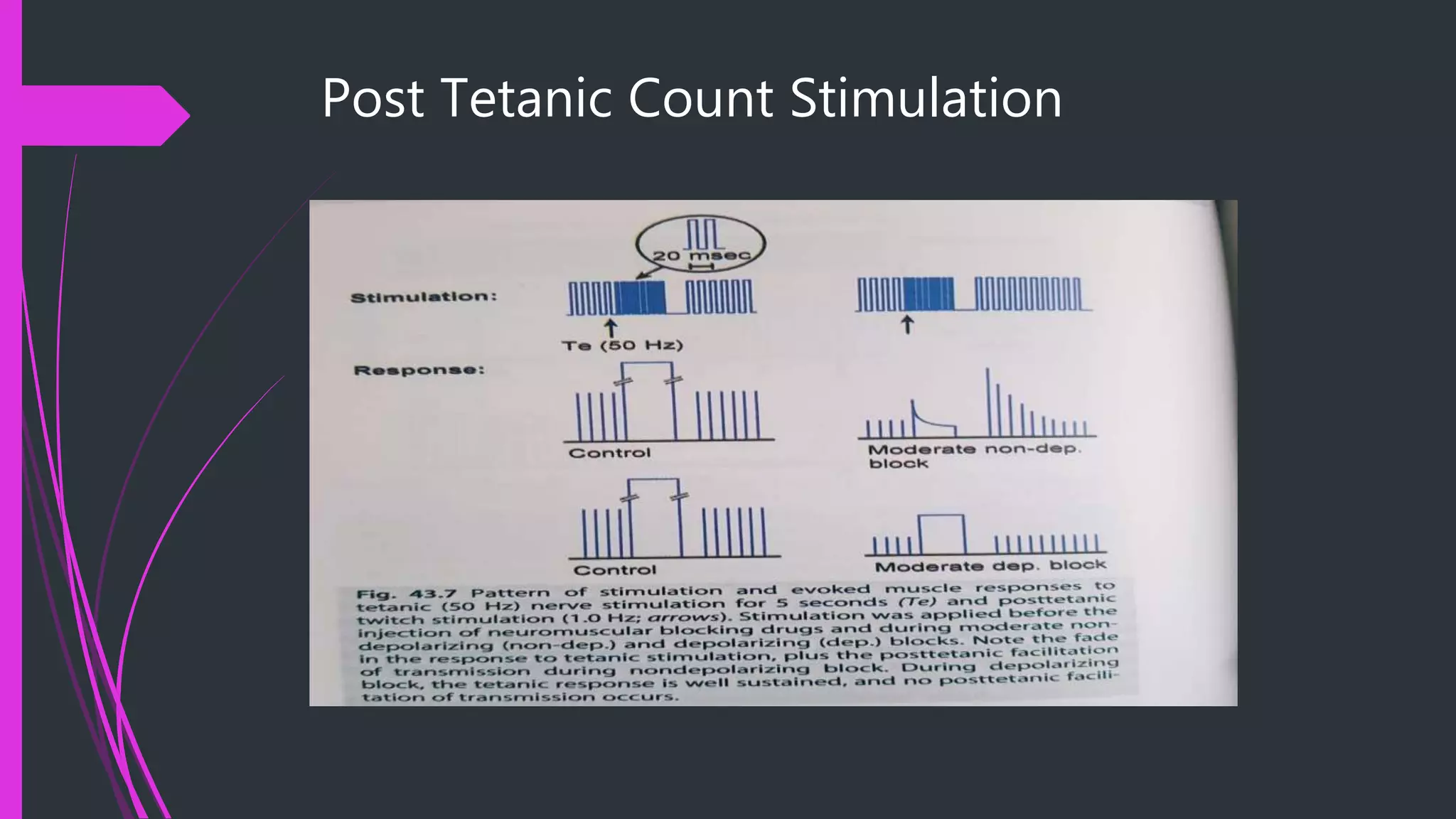
Post Tetanic CountStimulation
Stimulation Pattern
A composite stimulation pattern consisting of tetanic stimulation of 50 Hz for 5 seconds
followed by 10 t 15 single twitches given at 1 Hz starting at 3 seconds past the tetanic
stimulation.
Clinical application
When dense neuromuscular paralysis is required.
Onset (deep paralysis—less than 3 post tetanic count.
Surgical paralysis
Recovery( although painful but ideal).
Subjective monitor
Peripheralnerve stimulator: only allows the stimulation of the target nerve;
subsequent muscular response is evaluated subjectively (tactilely or visually).
27.
Objective Monitors
Mechanomyography:
Evoked mechanical response of the muscle.
gold standard technique.
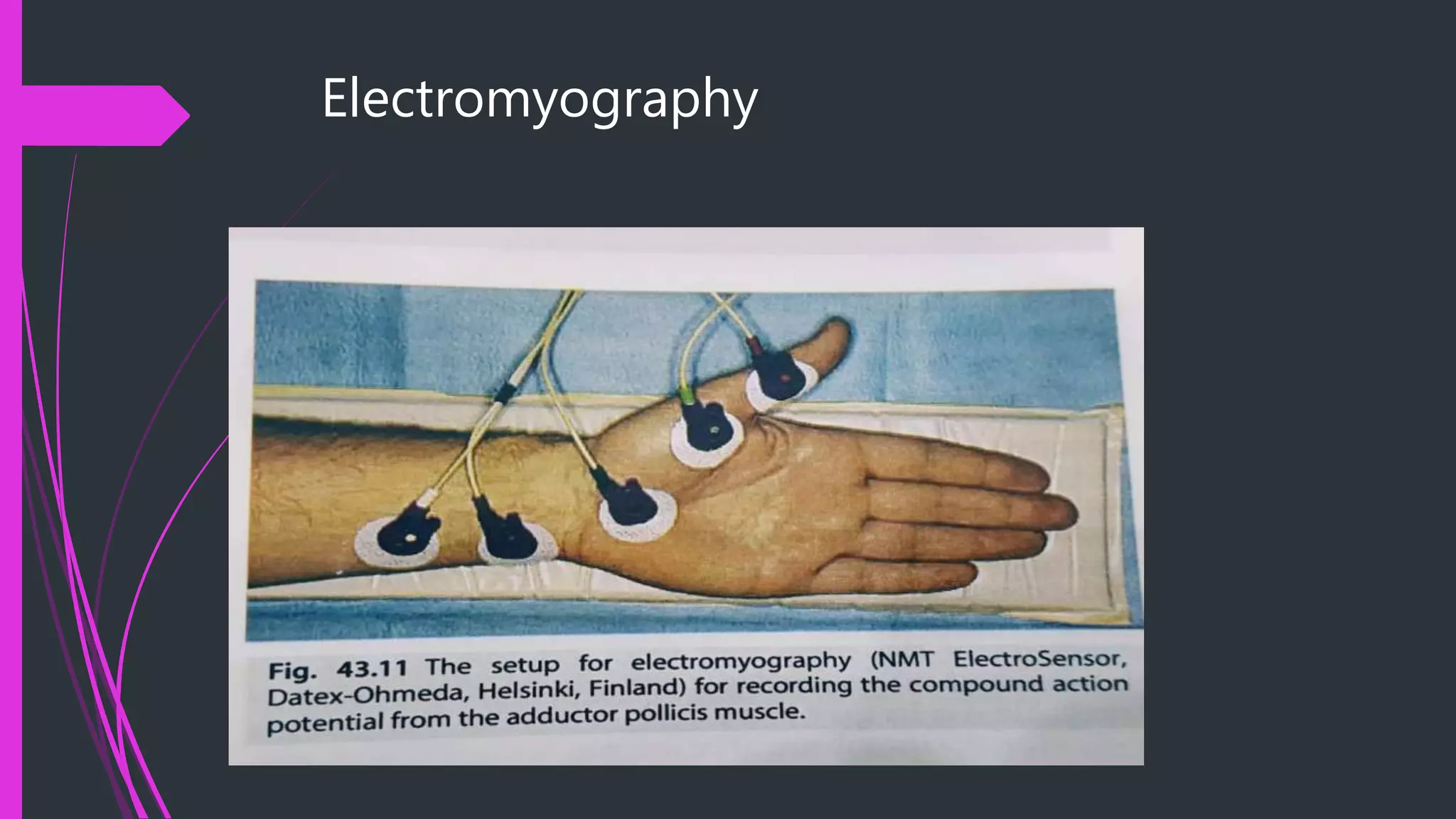
Electromyography:
Evoked electrical response of the muscle
Oldest method
Acceleromyography:
Acceleration of musv;le response
Based on newton’s second law i.e. Force= Mass X acceleration.
Kinemyography:
Evoked electrical response in a flexible piezoelectric film sensor attatched to the muscle.
Cuff pressure modality:
Measurement of pressure changes in BP Cuff after contaction of upper arm muscles.
Compressomyography:
measurement of a spherical balloon after hand contraction
Evaluation Of RecordedEvoked Responses with Non-
Depolarizing NMBA
Intense Block
Onset: within 3 to 6 minutes of intubating dose.
Also called ‘period of no response’.
Can only be antagonized by sugammadex high dose 16mg/kg.
Deep block
Intense block is followed by deep block.
Absence of response to TOF but with 1 PTC.
Assured by PTC less than and equal to 3 in laparoscopic surgeries.
Can only be reversed by sugammadex moderate dose 4mg/kg.
33.
Evaluation Of RecordedEvoked Responses with
Non-Depolarizing NMBA
Moderate block
Begins with first response to TOF and gradual return of four stiuli of TOF.
When Ist TOF response reappears, degree of block is 90 to 95 %
When fouryth response to TOF reappears, degree of block is 60 to 85%.
Reversed with sugammadex low dose 2mg/kg.
Or by neostigmine if TOF ratio 0.7 or above.
Recovery from block
Return of fourth response to TOF
TOF ratio should be 0.9 with MMG or EMG and 1.0 with AMG to exclude residual blockade.
34.
Evaluation Of RecordedEvoked Responses
with Depolarizing NMBA
Phase I block
Occurs in patients given succinylcholine once or with normal plasma pseudocholinesterase levels and
genetics.
No fade
No post tetanic facilitation
TOF ratio 1.0
TOF count is either 4 or 0.
Phase II block
Occures with repeated doses or continuous infusion of succinylcholinein patients with normal
pseudocholinesterase levels and normal genetics or patients with abormal plama pseudocholinesterase
levels or abnormal genetics.
Fade occurs
TOF ratio is utilized to differentiate the phase I and phase II blockade.