Why NMJ monitoring?
To ensure ideal intubating conditions have been met after administration
of muscle relaxant.
To ensure ideal surgical conditions have been met intraoperatively.
To administer NMBA’s with appropriate dosing.
Prevention of residual neuromuscular blockade.
Surgical indications.
Prolonged Anaesthesia.
Presence of renal or hepatic diseases.
3.
Methods of neuromuscularmonitoring
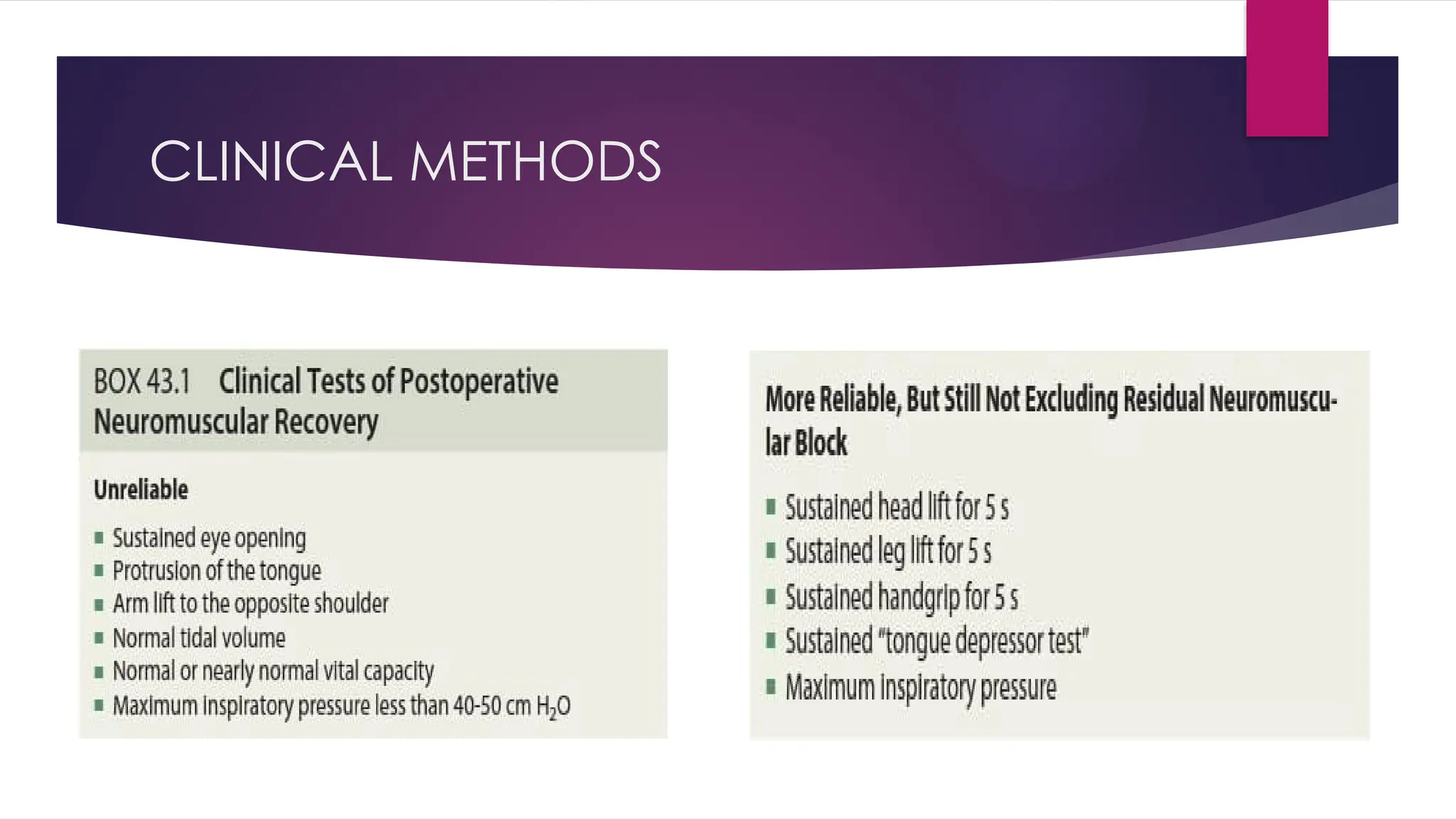
Clinical methods
Useful only towards the end of surgery for assessing recovery from NMB
Peripheral nerve stimulator
Subjective : visual / tactile
Objective : Quantification with numerical values
PERIPHERAL NERVE STIMULATOR
Evoking the response of muscle by delivering an electrical stimulus to the
nerve that innervates it.
Simple
Compact
Light weight
Stimulus – monophasic & rectangular wave form
Length of pulse – should not exceed 0.2 to 0.3 ms
Deliver constant current
6.
PERIPHERAL NERVE STIMULATOR
Stimulating electrodes
Surface electrodes (30-70mA)
Metal electrodes
Needle electrodes (10mA)
Current
Supramaximal stimulus – 25 % of maximal stimulus
Higher currents – oedema, diabetes
Lower currents – needle electrodes are used
DIFFERENT MUSCLES GROUPSHAVE
DIFFERENT SENSITIVITY TO NMBD’S
Diaphragm & laryngeal adductors, corrugator supercili – resistant to NMBD’S
Onset is late
Recovery is fast
Extrapolated by corrugator supercilii
Peripheral muscles of limbs, orbicularis oculi, upper airway muscles –
sensitive to NMBD’S
Onset is fast
Recovery is slow
Extrapolated by adductor pollicis
9.
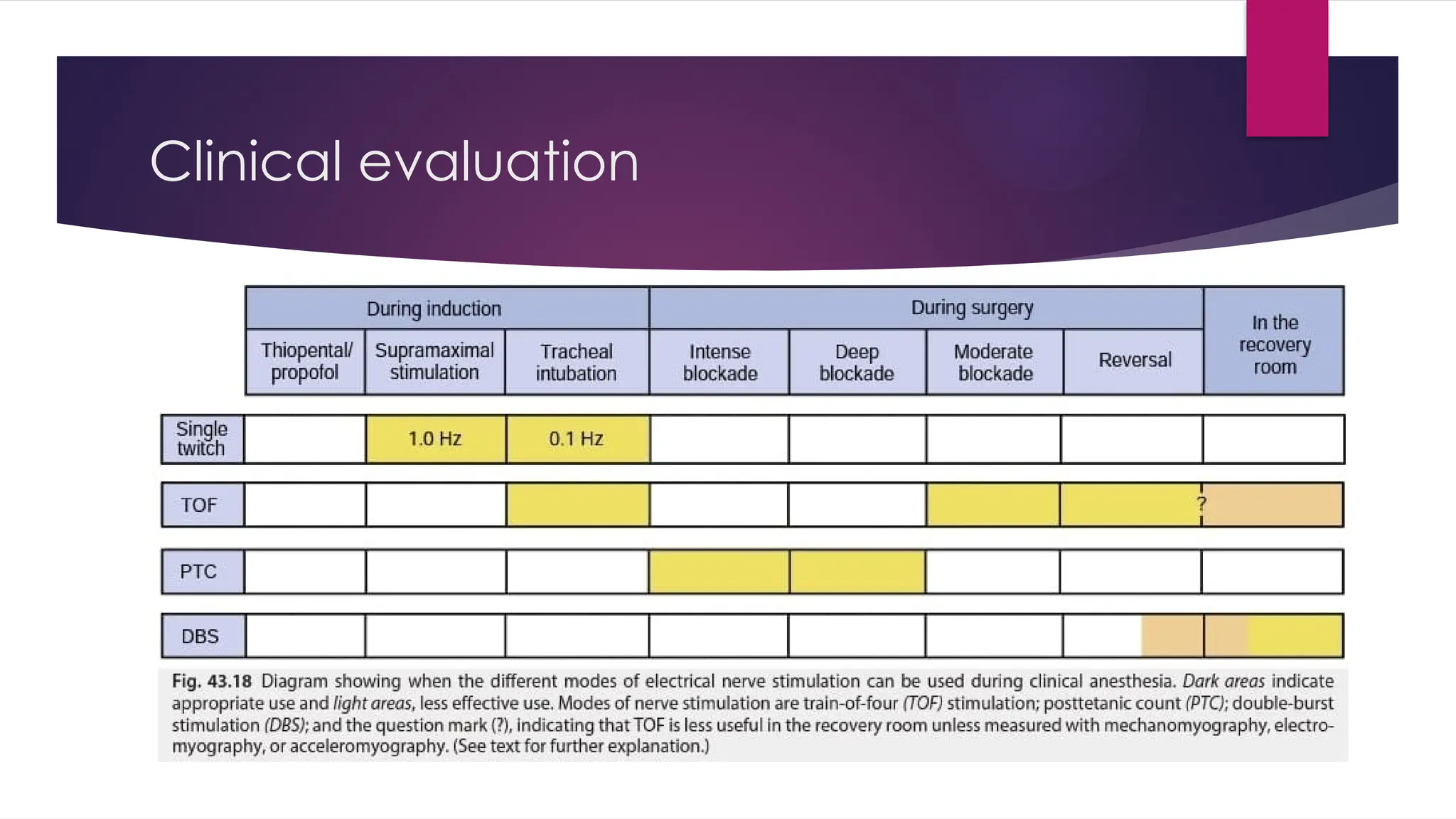
Patterns of nervestimulation
1. Single twitch stimulation
2. Train of four stimulation(TOF)
3. Double burst stimulation(DBS)
4. Tetanic stimulation
5. Post tetanic stimulation(PTC)
10.
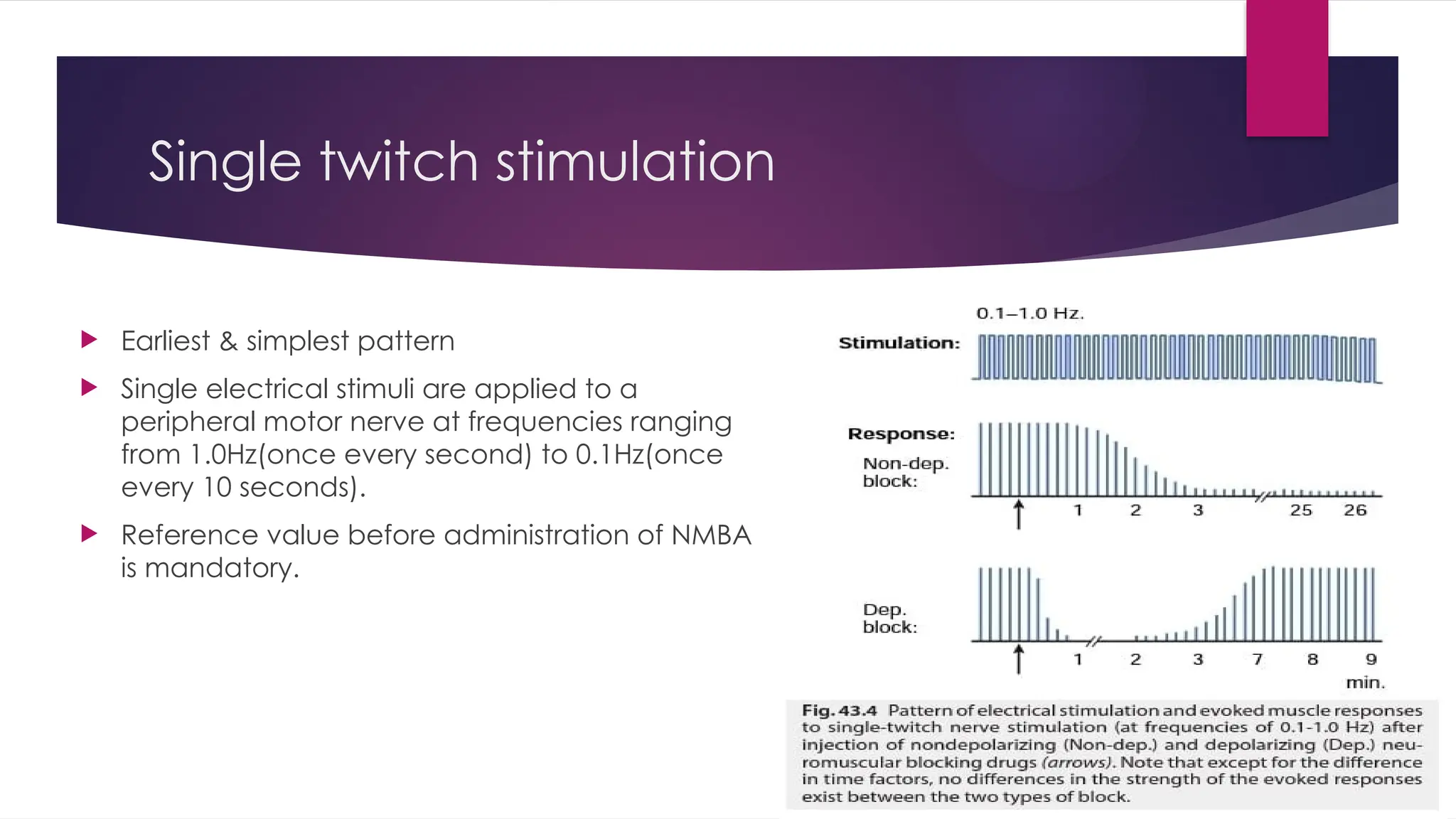
Single twitch stimulation
Earliest & simplest pattern
Single electrical stimuli are applied to a
peripheral motor nerve at frequencies ranging
from 1.0Hz(once every second) to 0.1Hz(once
every 10 seconds).
Reference value before administration of NMBA
is mandatory.
11.
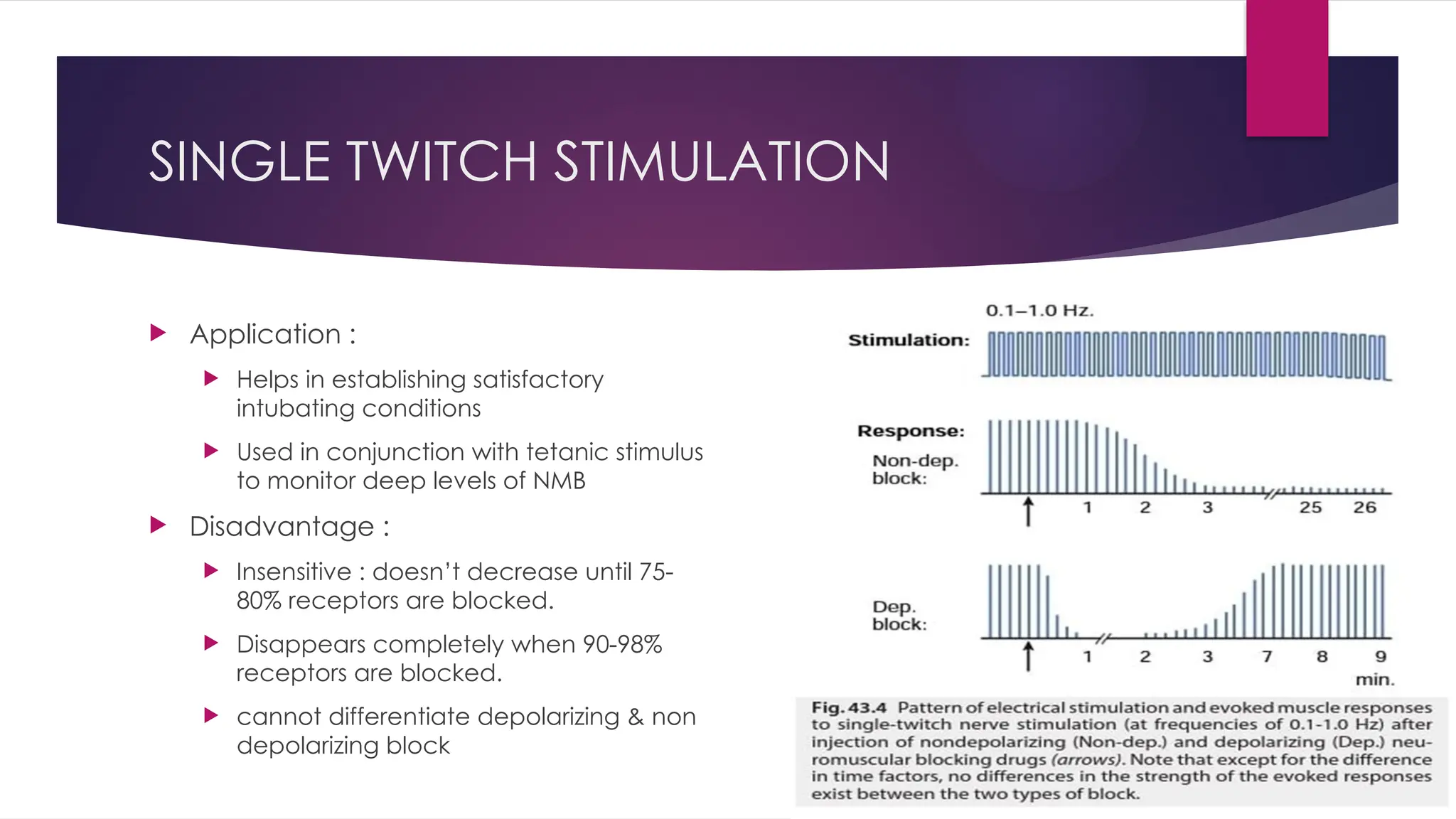
SINGLE TWITCH STIMULATION
Application :
Helps in establishing satisfactory
intubating conditions
Used in conjunction with tetanic stimulus
to monitor deep levels of NMB
Disadvantage :
Insensitive : doesn’t decrease until 75-
80% receptors are blocked.
Disappears completely when 90-98%
receptors are blocked.
cannot differentiate depolarizing & non
depolarizing block
12.
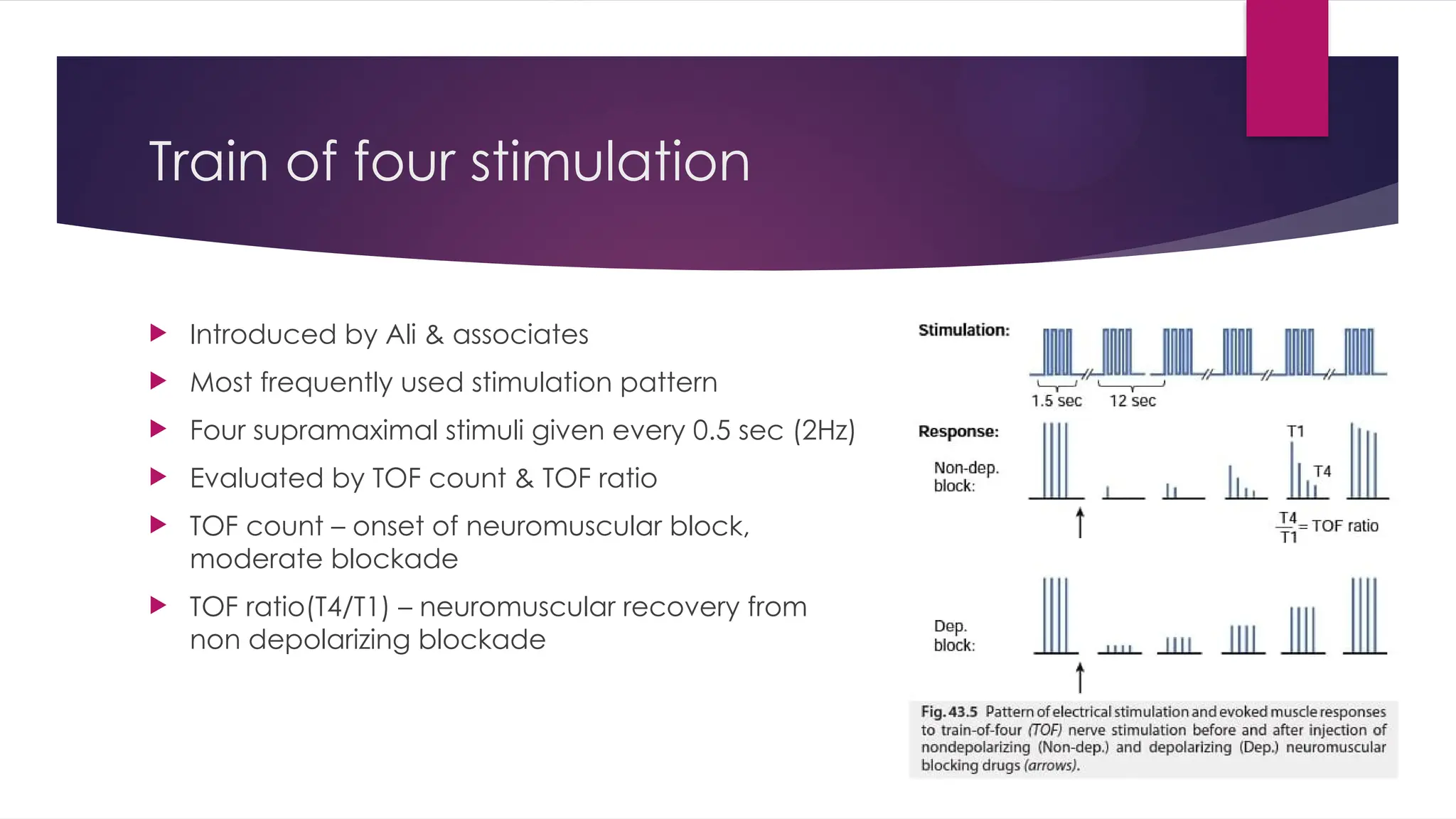
Train of fourstimulation
Introduced by Ali & associates
Most frequently used stimulation pattern
Four supramaximal stimuli given every 0.5 sec (2Hz)
Evaluated by TOF count & TOF ratio
TOF count – onset of neuromuscular block,
moderate blockade
TOF ratio(T4/T1) – neuromuscular recovery from
non depolarizing blockade
13.
TRAIN OF FOUR
Degree of fade is proportional to extent of neuromuscular block
At unblocked NMJ, TOF ratio equals to 1.0
Phase 1 block of depolarizing muscle relaxants, twitch height is decreased in all four twitches,
( no fade and TOF ratio equals to 1.0)
Phase 2 block of depolarizing muscle relaxants or block of NDMR T4 height starts to decrease
when 70-75% receptors are blocked, while T1 remains same ( fade and TOF ratio equals to 0.7
80% receptors are blocked – 4th
twitch disappears
85% receptors are blocked – 3rd
twitch disappears
90% receptors are blocked – 2nd
twitch disappears
>90% receptors are blocked – 1st
twitch disappears
14.
TOF
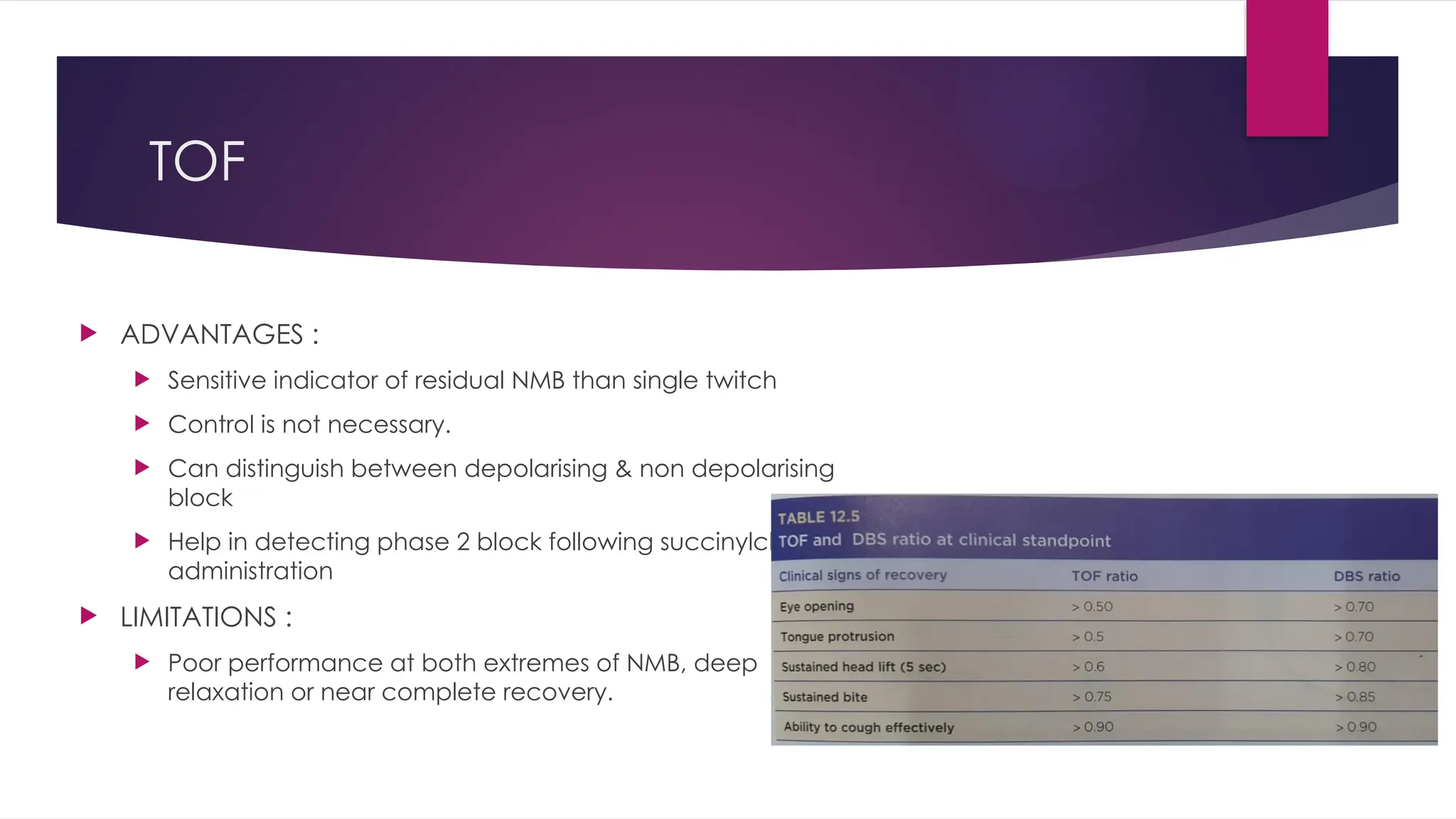
ADVANTAGES :
Sensitive indicator of residual NMB than single twitch
Control is not necessary.
Can distinguish between depolarising & non depolarising
block
Help in detecting phase 2 block following succinylcholine
administration
LIMITATIONS :
Poor performance at both extremes of NMB, deep
relaxation or near complete recovery.
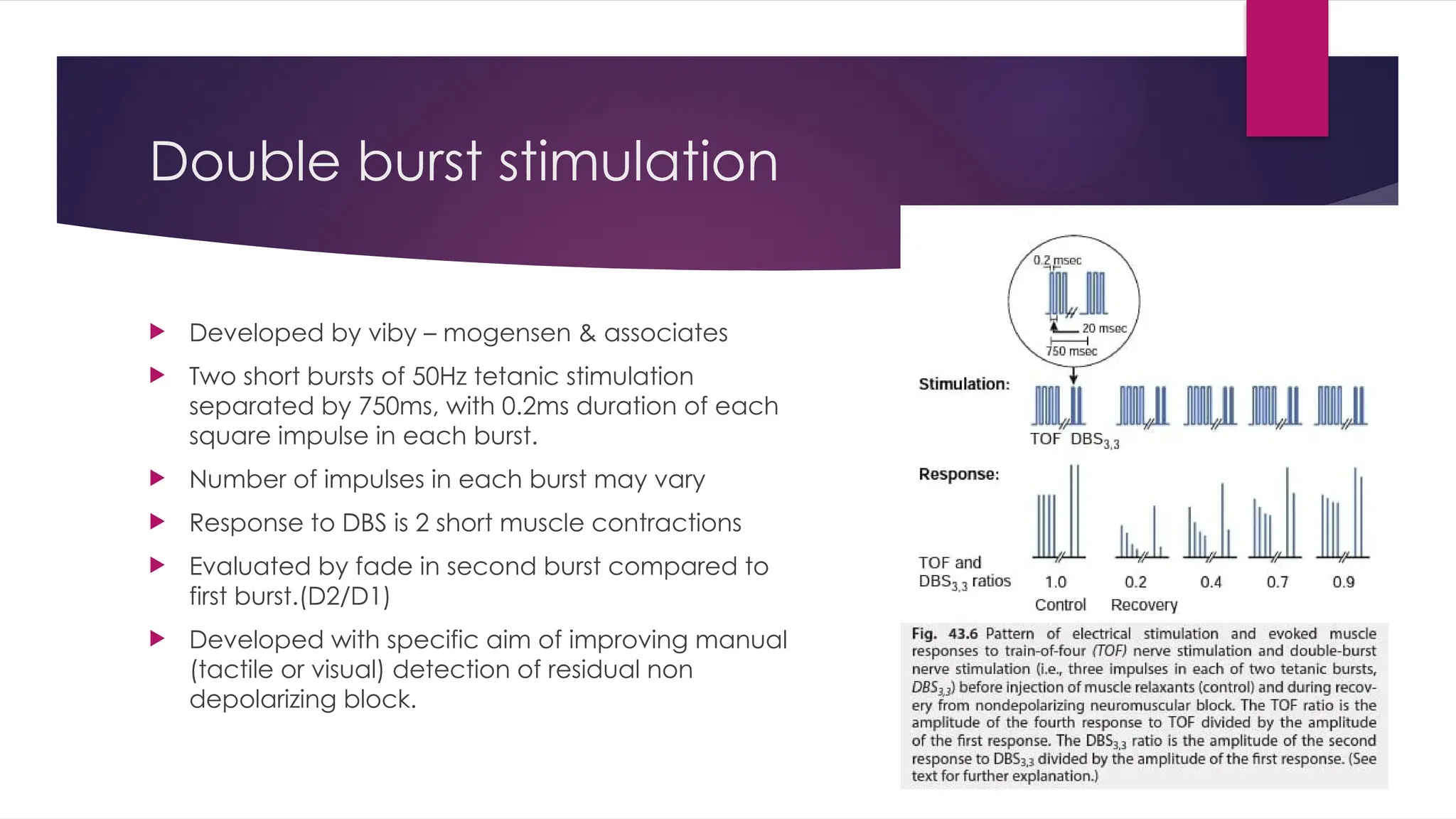
Double burst stimulation
Developed by viby – mogensen & associates
Two short bursts of 50Hz tetanic stimulation
separated by 750ms, with 0.2ms duration of each
square impulse in each burst.
Number of impulses in each burst may vary
Response to DBS is 2 short muscle contractions
Evaluated by fade in second burst compared to
first burst.(D2/D1)
Developed with specific aim of improving manual
(tactile or visual) detection of residual non
depolarizing block.
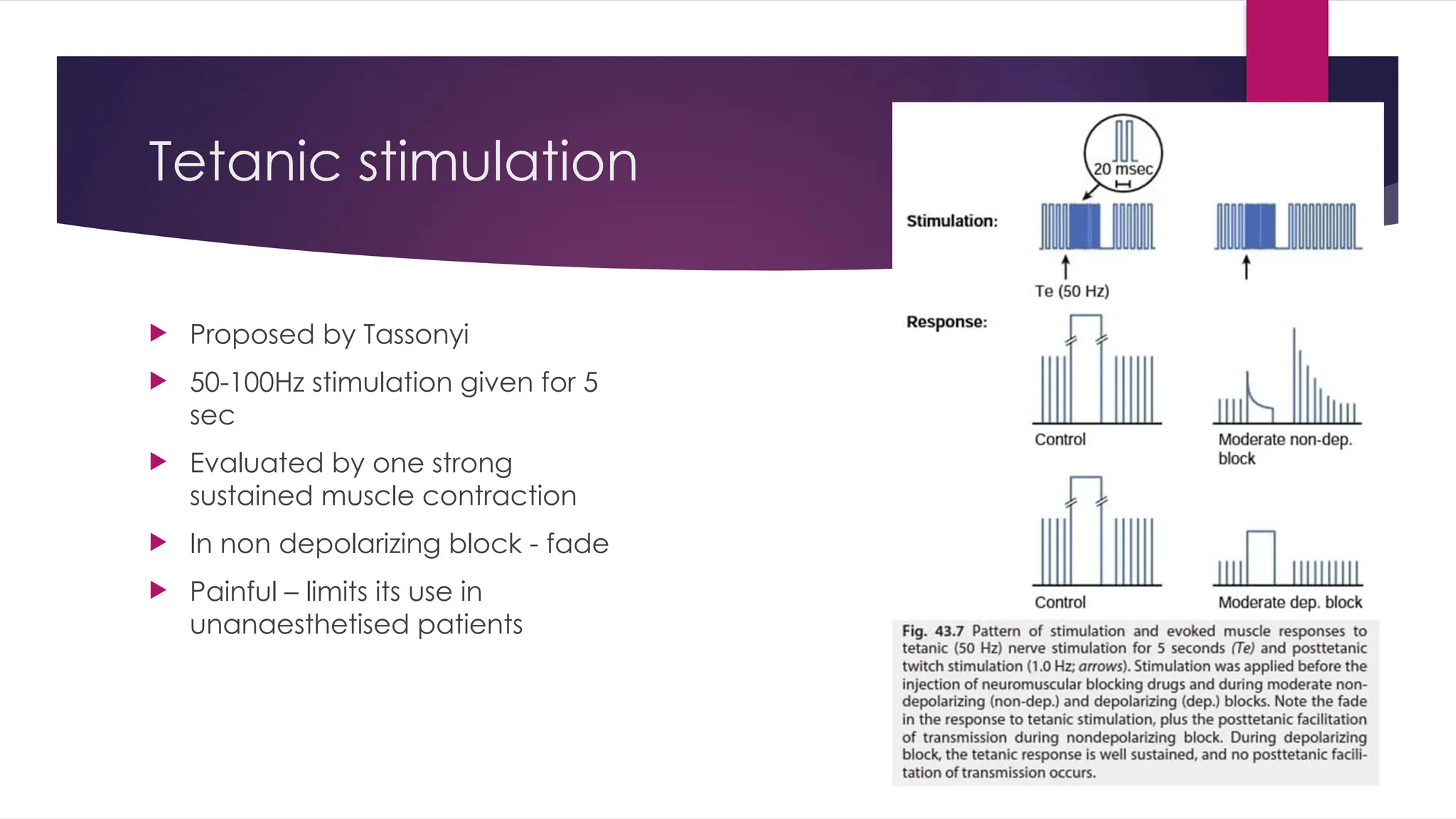
Tetanic stimulation
Proposedby Tassonyi
50-100Hz stimulation given for 5
sec
Evaluated by one strong
sustained muscle contraction
In non depolarizing block - fade
Painful – limits its use in
unanaesthetised patients
19.
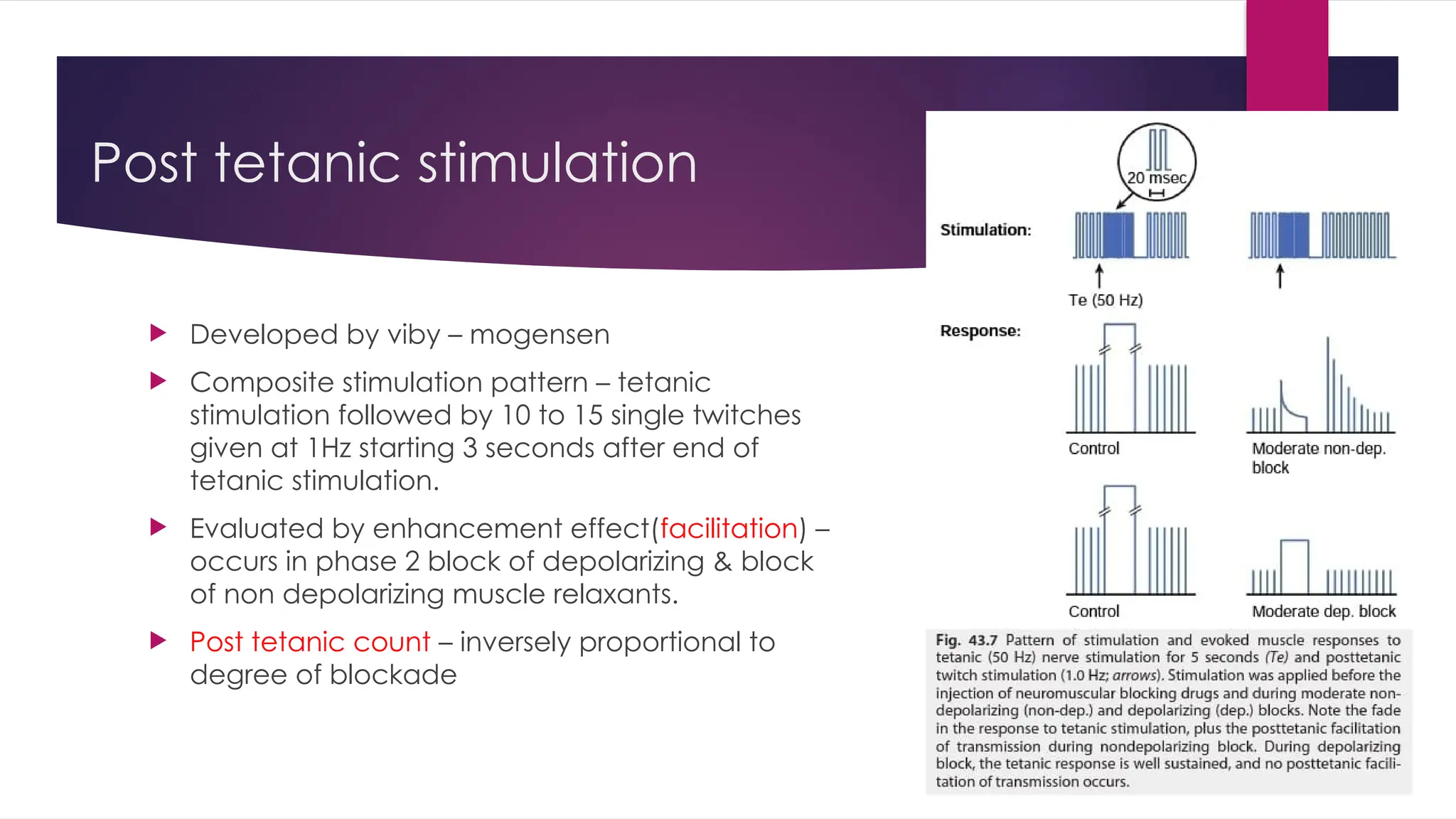
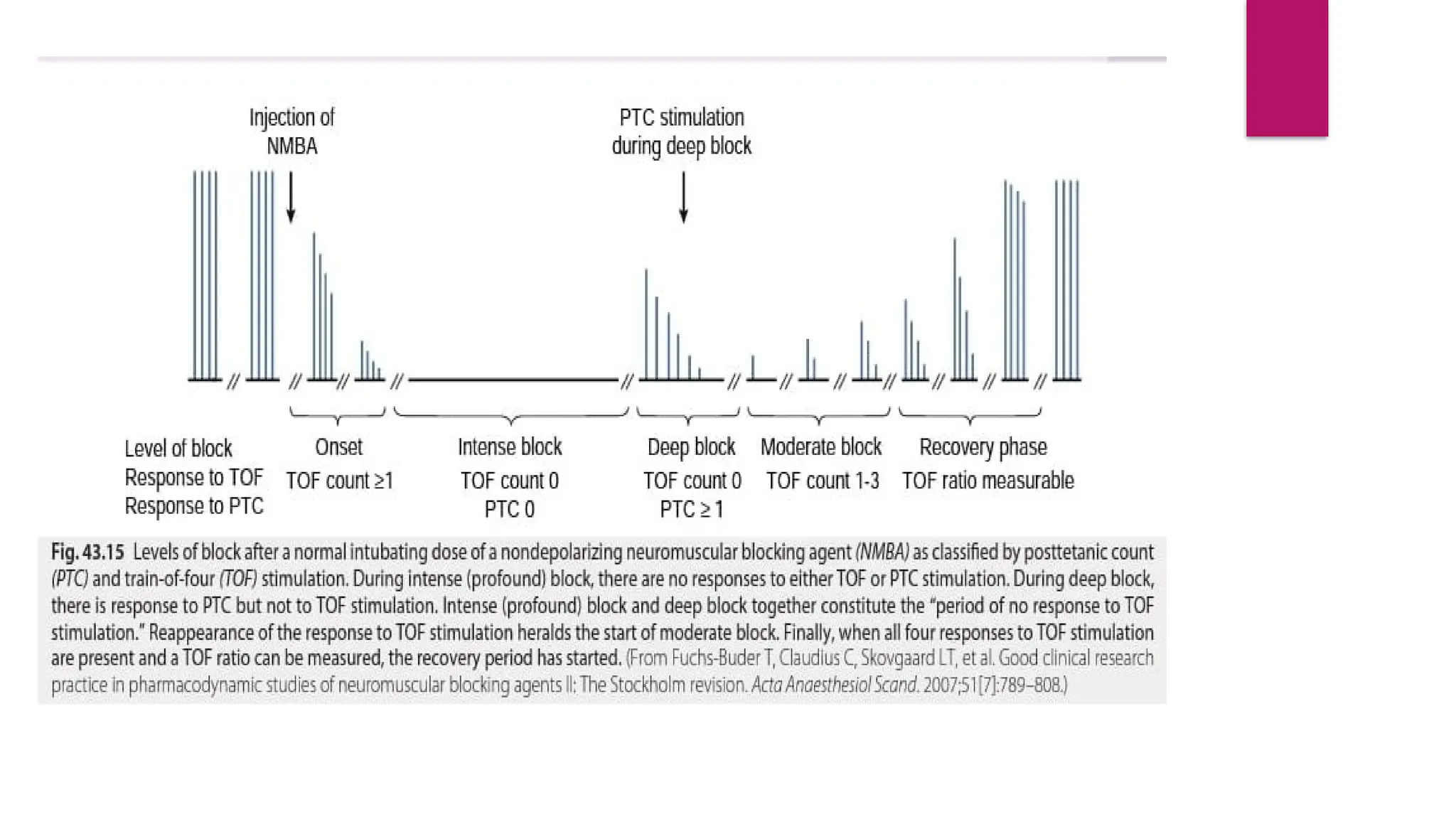
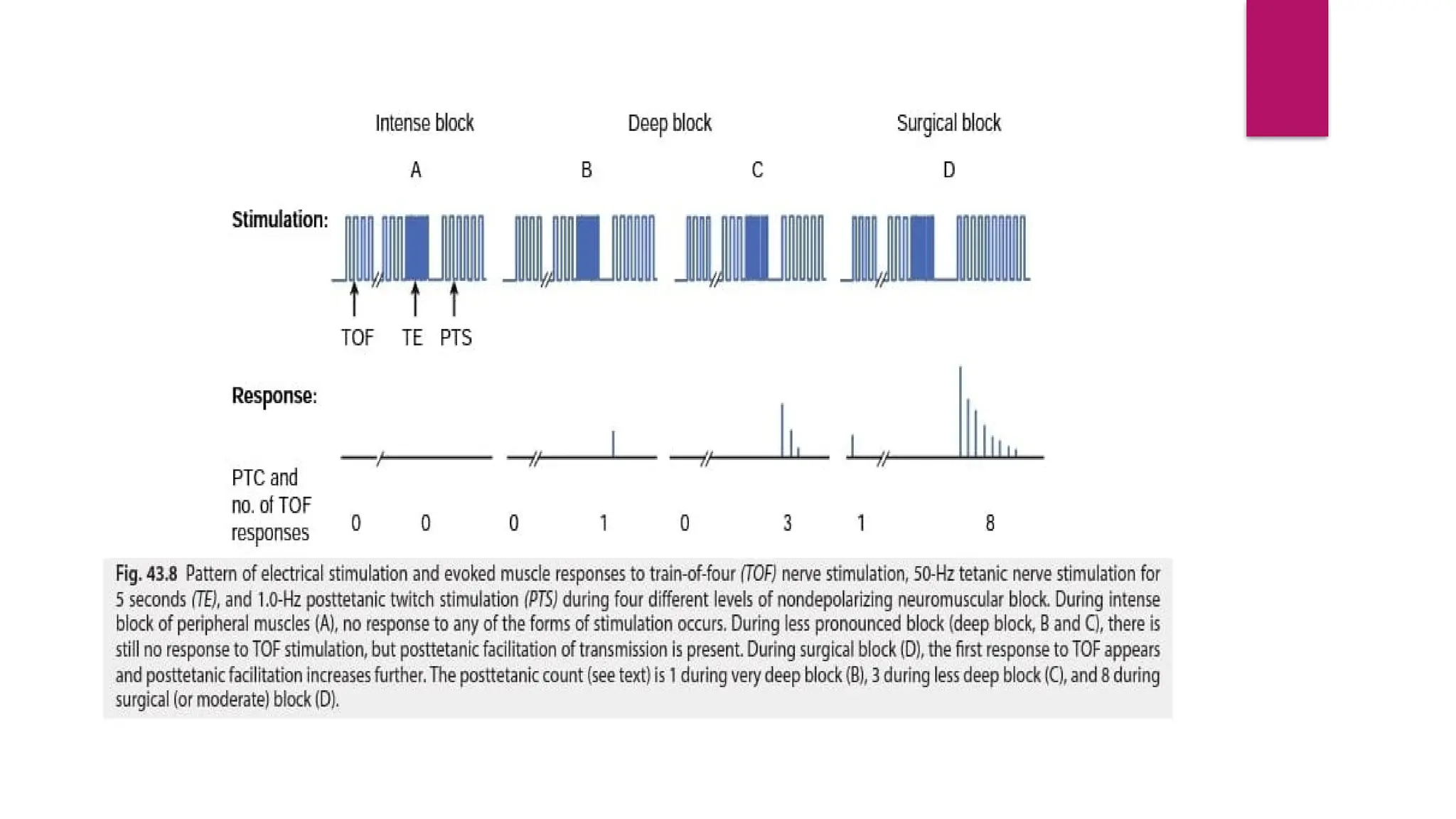
Post tetanic stimulation
Developed by viby – mogensen
Composite stimulation pattern – tetanic
stimulation followed by 10 to 15 single twitches
given at 1Hz starting 3 seconds after end of
tetanic stimulation.
Evaluated by enhancement effect(facilitation) –
occurs in phase 2 block of depolarizing & block
of non depolarizing muscle relaxants.
Post tetanic count – inversely proportional to
degree of blockade
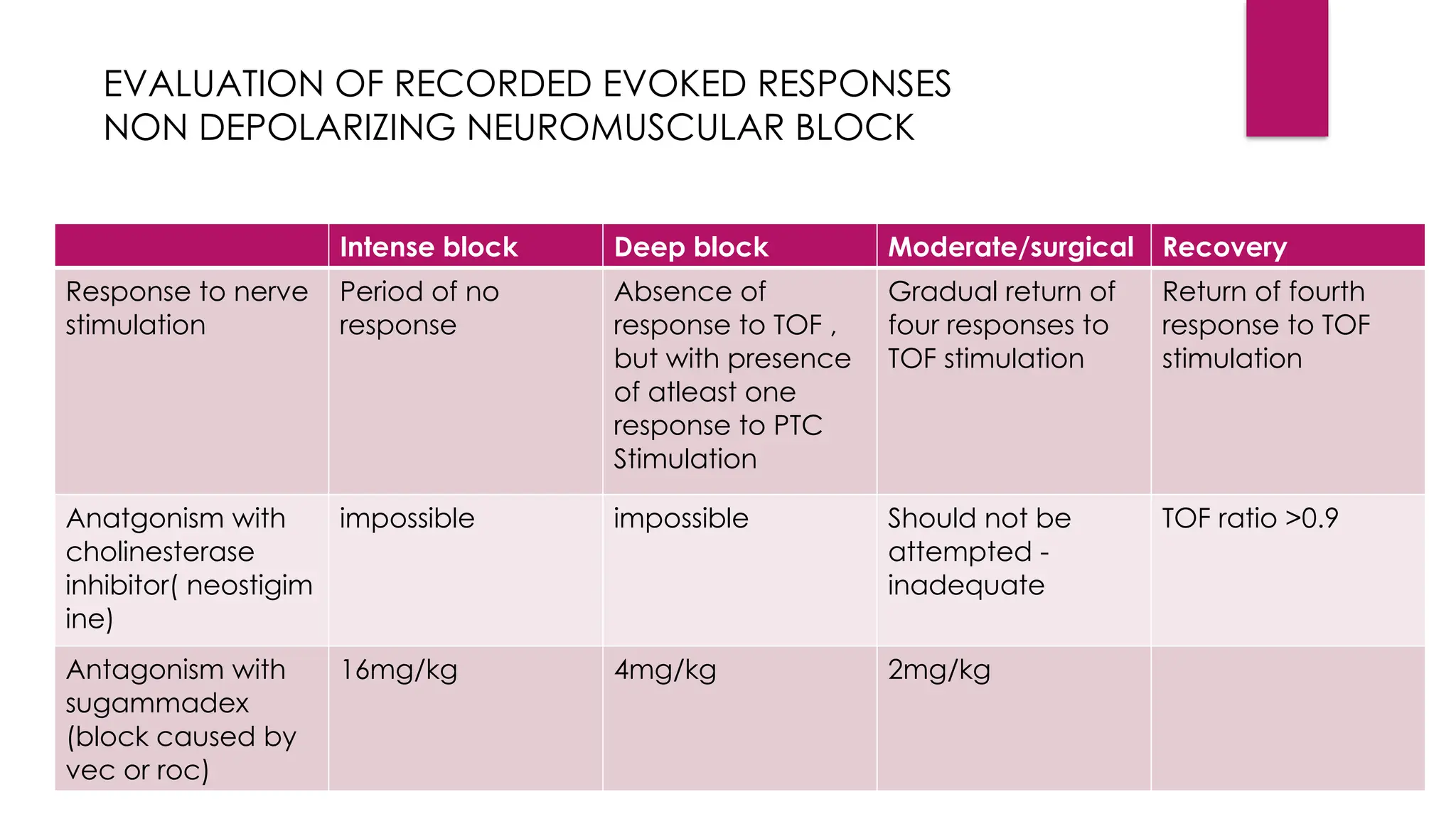
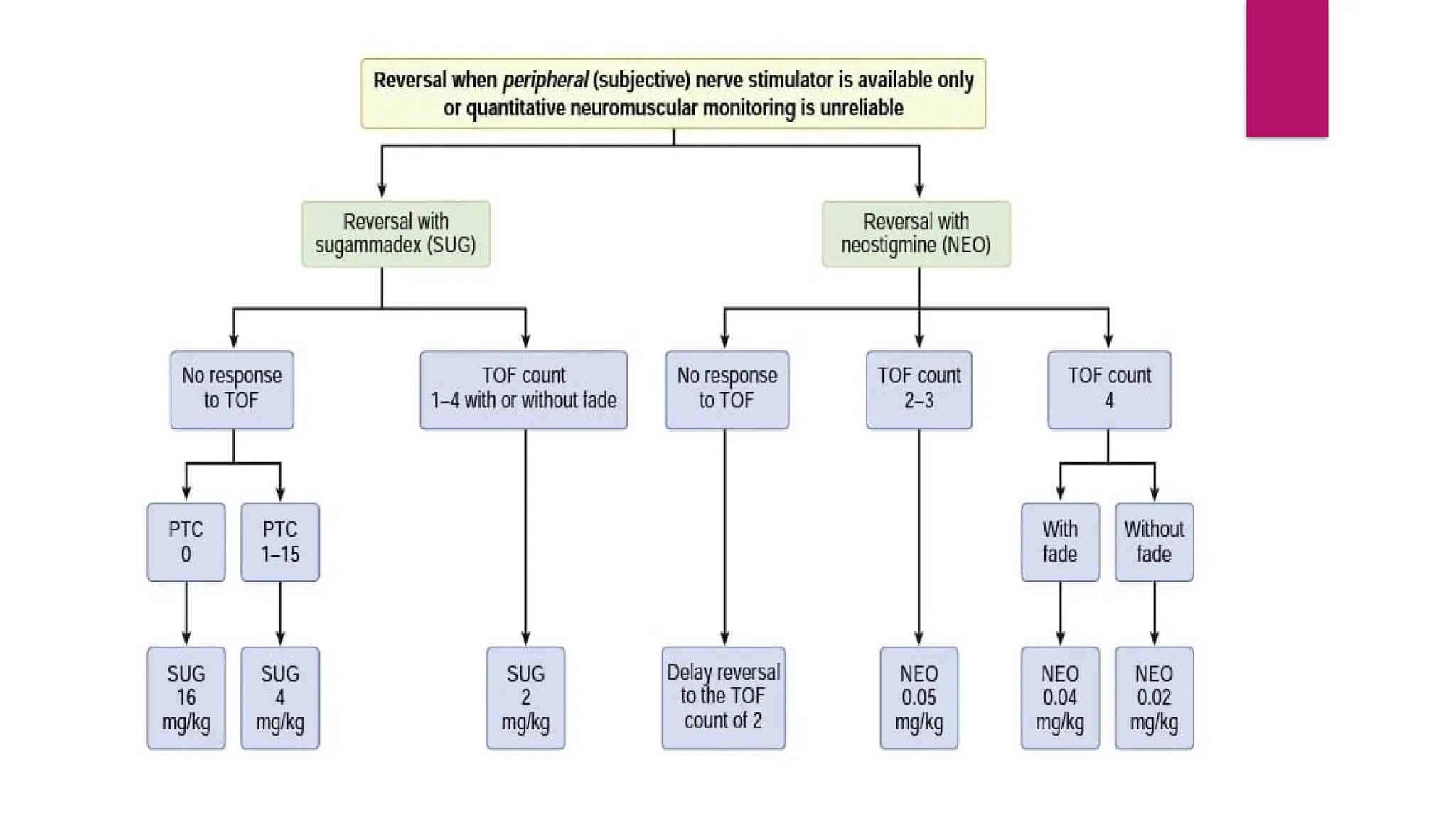
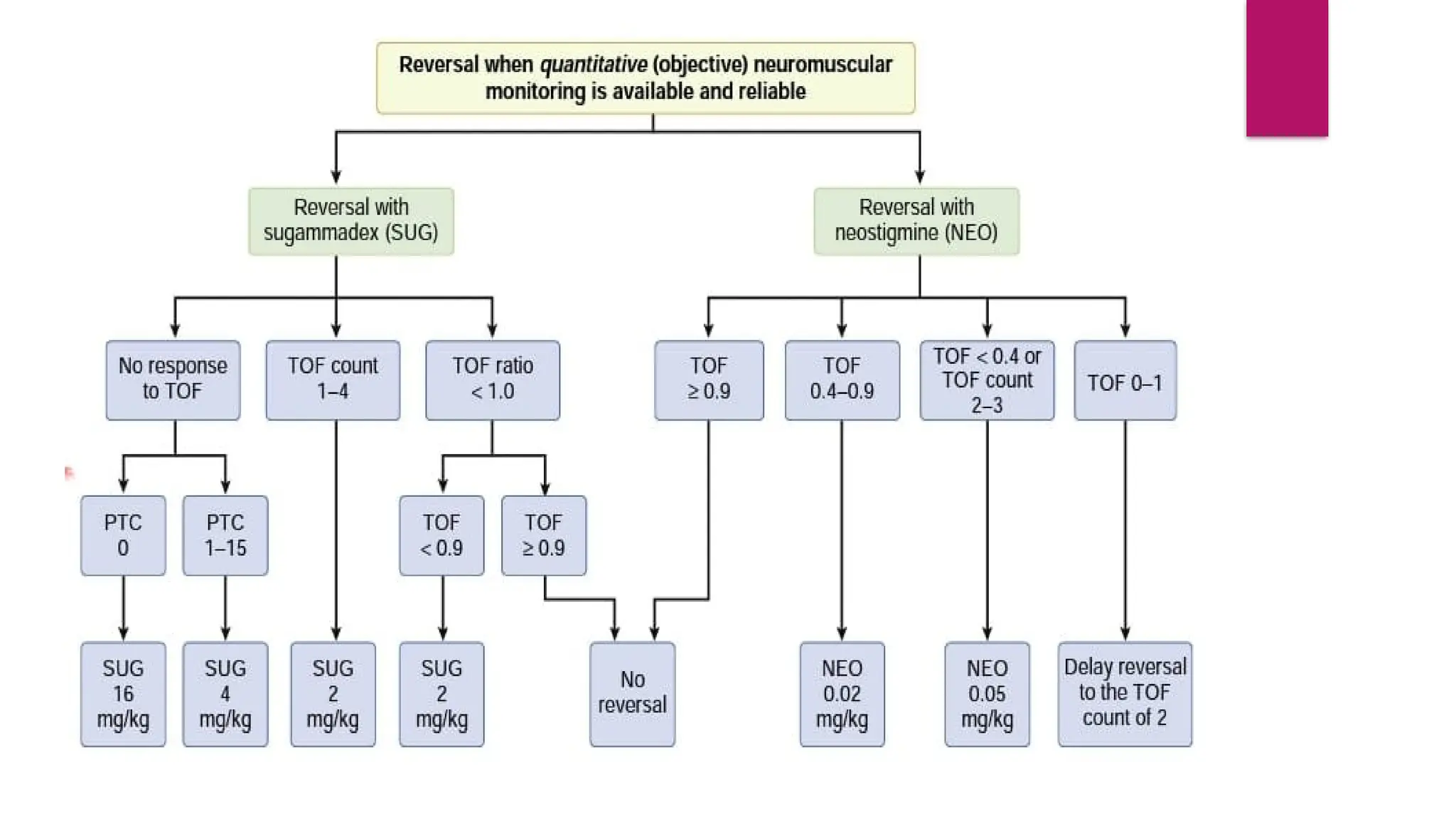
Intense block Deepblock Moderate/surgical Recovery
Response to nerve
stimulation
Period of no
response
Absence of
response to TOF ,
but with presence
of atleast one
response to PTC
Stimulation
Gradual return of
four responses to
TOF stimulation
Return of fourth
response to TOF
stimulation
Anatgonism with
cholinesterase
inhibitor( neostigim
ine)
impossible impossible Should not be
attempted -
inadequate
TOF ratio >0.9
Antagonism with
sugammadex
(block caused by
vec or roc)
16mg/kg 4mg/kg 2mg/kg
EVALUATION OF RECORDED EVOKED RESPONSES
NON DEPOLARIZING NEUROMUSCULAR BLOCK
24.
DEPOLARIZING NEUROMUSCULARBLOCK
Phase 1 block : response to TOF or tetanic stimulation does not fade, no
posttetanic facilitation
Phase 2 block : fade in response to TOF & tetanic stimulation & post tetanic
facilitation
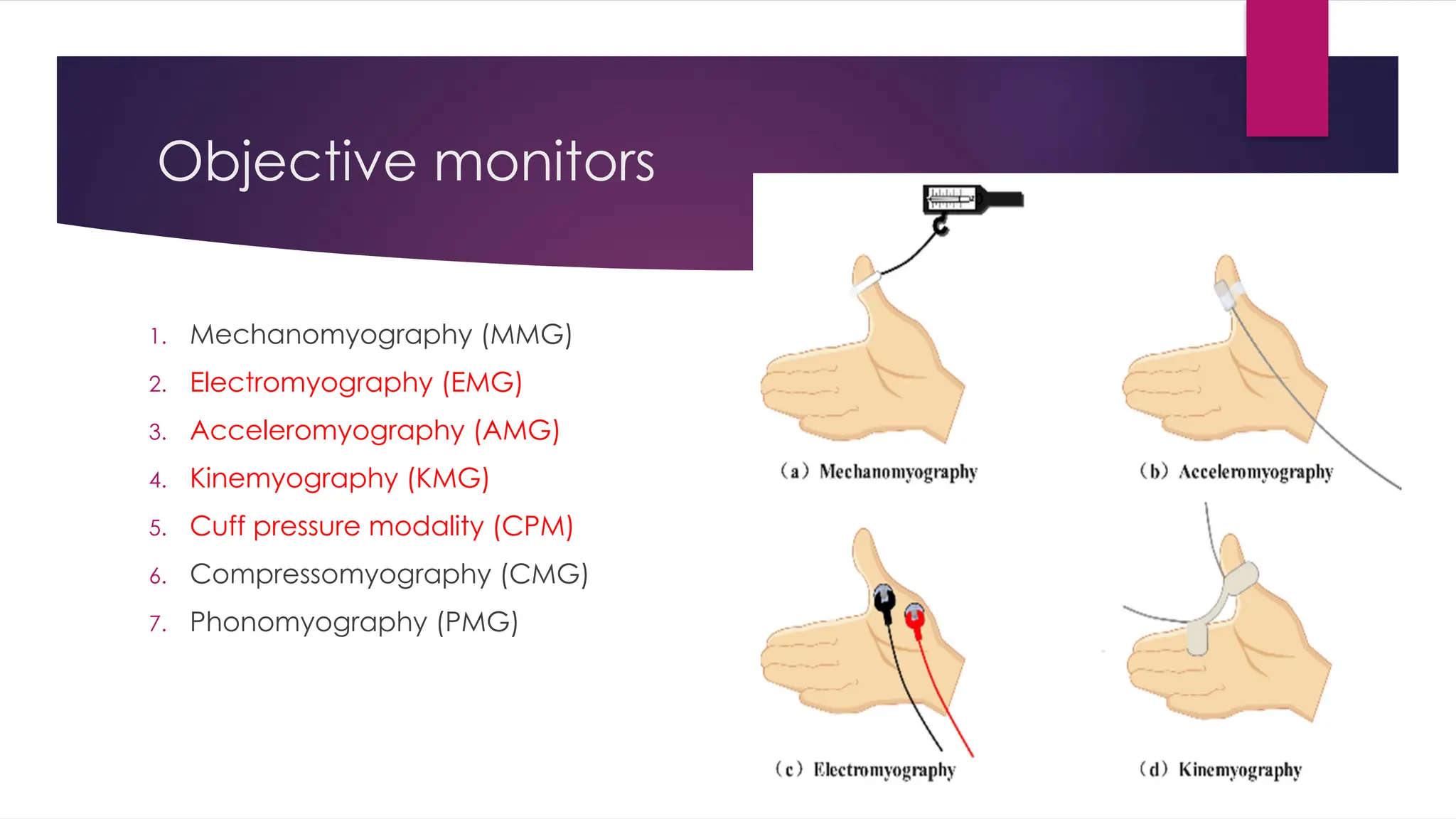
Mechanomyography
Measuresthe isometric contraction of muscle after stimulation of corresponding
nerve.
Electromyography
Records the compound muscle action potentials produced by stimulation of
peripheral nerve.
Acceleromyography
Records the isotonic acceleration of stimulated muscle
29.
Kinemyography
Stretching/bending of flexible piezoelectric film in response to nerve stimulation
generates a voltage that is proportional to amount of stretching or bending.
Cuff pressure modality (CPM)
Detects changes in cuff pressure due to muscle contractions.
Compressomyography
Measures pressure changes in a hand held balloon,
Phonomyography
Measures intrinsic low frequency sounds of muscle contractions with special
microphones following nerve stimulation
31.
Role of neuromuscularmonitoring in
neuromuscular diseases
Myasthenia gravis –
Down regulation of Ach receptors
Resistant to succinyl choline – requires more dose
Sensitive to NDMR – 50 -75% decrease in dose
Before giving NDMR – TOF ratio <0.9 – more sensitive to NMDR
Hemiplegia
Upregulation of AchRs
Increased dosage of NDMR