Downloaded 13 times
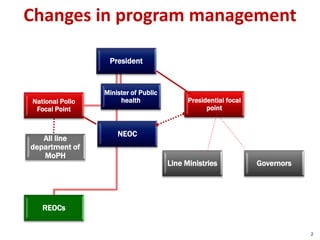
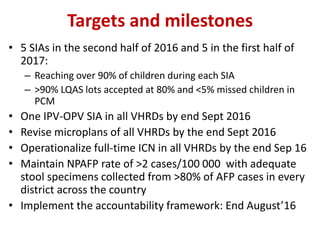
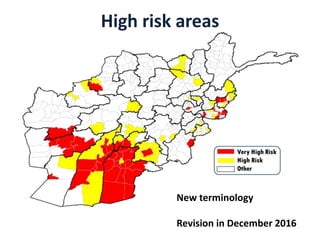
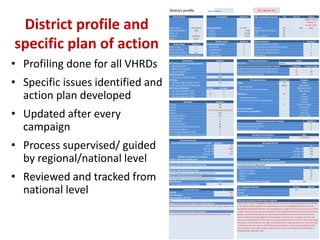
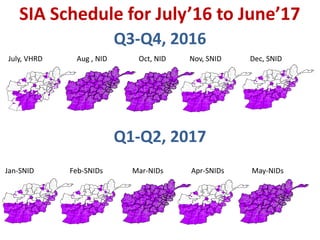
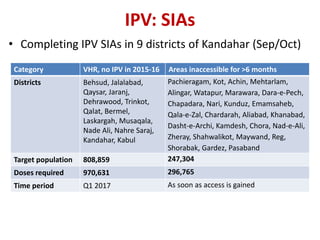
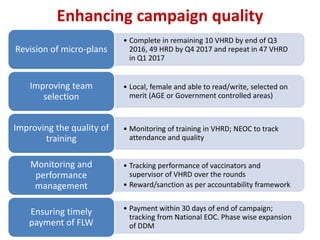
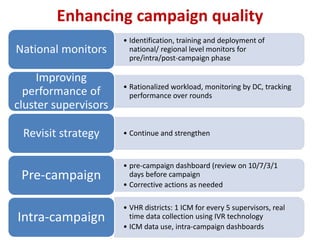
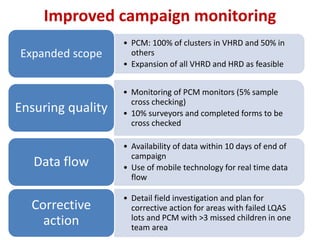
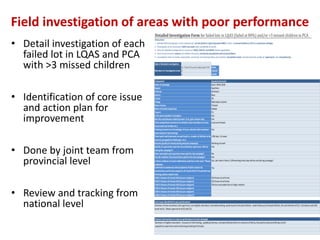
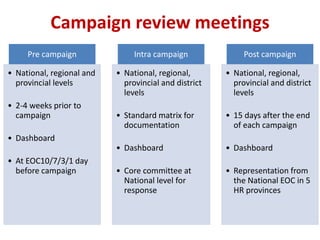
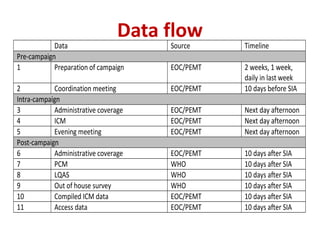


This document outlines Afghanistan's National Emergency Action Plan (NEAP) for polio eradication from 2016-2017. The plan's goal is to stop wild poliovirus transmission in Afghanistan by the end of 2016 with no new cases in 2017. Key strategies include maintaining program neutrality, focusing on high-risk areas, strengthening community engagement, and enhancing accountability. Targets include conducting 10 vaccination campaigns in 2016-2017 and improving surveillance. The plan also discusses improving campaign quality, monitoring, and data collection to enhance polio eradication efforts.























































































